Application of Carl Rogers' Theories to Males
In a 2023 internal audit at a Midwestern VA hospital, clinicians documented that 71 of 73 male veterans formally diagnosed with PTSD scored in the “low emotional expressiveness” range on the Berkeley Expressivity Questionnaire, yet 64 of them reported somatic complaints averaging 11.3 primary‑care visits per year—an incongruence strikingly consistent with Carl Rogers’ predictions about denied affect. This pattern emerged despite all patients having completed at least one manualized, symptom‑focused treatment protocol.
Such data sit uneasily beside Rogers’ assumption of an actualizing tendency that unfolds in the presence of unconditional positive regard, because contemporary masculinity norms appear to recalibrate conditions of worth around invulnerability, performance, and self‑suppression. Consequently, the male self‑concept is frequently organized less around subjective experience than around compliance with externally validated competency scripts.
The complexity of applying a person‑centered framework to male clients becomes evident in microprocess research. In a 2019 session‑coding study at the Men’s Counseling Clinic at the University of Missouri, sessions with predominantly male caseloads exhibited a 38% higher rate of “deflecting humor” responses immediately following empathic reflections than mixed‑gender samples, a finding that suggests defensive operations precisely at the moment of offered relational depth. According to Michael Addis, PhD, whose work on masculinities and help‑seeking behavior at Clark University has been central to this field, such patterns “represent not resistance to therapy per se, but loyalty to an internalized masculine audience.” First‑session recordings from a London IAPT service in March 2022—where 82% of male clients spontaneously apologized when expressing sadness—further indicate that the translation of Rogers’ core conditions into male‑socialized subjectivities remains an unresolved, empirically tractable problem of contemporary clinical practice.
Core Principles of Person‑Centered Theory
A critical yet underexamined principle in Rogers’ work, especially with male clients, is the locus of evaluation—the gradual shift from externalized performance criteria toward an internally referenced phenomenological standard.
First, this construct matters because male socialization frequently embeds an overlearned external locus of evaluation: occupational rank, athletic success [1], [2], or relational control function as de facto conditions of worth, constraining access to vulnerable affect and authentic preference. In such cases, unconditional positive regard does not simply “accept” the client; it systematically disrupts the client’s internalized evaluative audience.
Clinically, this shift can be mapped as a process: initial reliance on external metrics (e.g., promotions at Goldman Sachs or deployment commendations in the U.S. Army), followed by destabilization when empathic reflection exposes the emotional costs of those metrics, and culminating, where therapy is effective, in the emergence of idiosyncratic values that no longer mirror hegemonic masculinity. Outcome data from person‑centered men’s groups at the University of Wisconsin–Madison Counseling Psychology Clinic, where male participants reported reduced self‑silencing on session‑by‑session process measures, suggest that this sequence is neither incidental nor rare.
As John C. Norcross, PhD, has argued in his work on psychotherapy relationships, treatment outcome consistently covaries with “the client’s increasing reliance on internal rather than delegated standards of value.”
“The maturation of an internal locus of evaluation is arguably the most robust common factor across experiential therapies.”
— John C. Norcross, PhD, Distinguished Professor of Psychology, University of Scranton
A useful heuristic here is the evaluative pivot: the moment a male client spontaneously references “what feels right to me” rather than “what I am supposed to do.” That pivot, rather than symptom reduction alone, may constitute the most valid operationalization of Rogers’ core principles for male populations.
Understanding the Actualizing Tendency
A central but frequently misapplied element of Rogers’ actualizing tendency in male clients is its directionality: it operates not as a vague drive toward “growth,” but as a continual micro‑selection of experiences that move the organism away from shame and toward viability in a gendered evaluative field.
First, when masculinity norms define viability in terms of control and invulnerability, the actualizing tendency often expresses itself through defensive competence—overwork, hyper‑independence, or somatization—rather than through explicit emotional exploration. The process is not a failure of the tendency but a context‑bound optimization problem: the self reorganizes toward what appears most compatible with survival in a particular masculine hierarchy.
Comparatively, cognitive–behavioral frameworks tend to interpret such patterns primarily as maladaptive schemas, whereas a strict person‑centered formulation treats them as best‑available strategies generated by an intact organismic valuing process under distorted conditions of worth. The former permits more rapid symptom modification; the latter offers a more coherent account of why symptoms often reconfigure rather than resolve in men whose external mandates remain unchanged.
An original and clinically useful distinction is between protective actualization (growth in the service of maintaining an unassailable masculine persona) and experiential actualization (growth that prioritizes the accuracy of felt experience over social legibility). In practice, the transition between these modes can be observed in small but reliable shifts in language, from third‑person generalizations (“men just have to suck it up”) to first‑person, affect‑laden statements.
In a 2021 outcome review at the Veterans Outreach Center in Rochester, New York [3], male participants in a person‑centered group program who demonstrated this linguistic shift by week four showed a 29% greater reduction in CORE‑OM global distress scores over 12 weeks than those who did not, despite identical session dosage and facilitator training, suggesting that mode of actualization may be a more sensitive process indicator than diagnosis or symptom count.
As Mick Cooper, PhD, Professor of Counselling Psychology at the University of Roehampton, has argued,
“The question is not whether clients actualize, but what they are being forced to actualize toward in the ecological niche they inhabit.”
— Mick Cooper, PhD, Professor of Counselling Psychology, University of Roehampton
The actualizing tendency in men, therefore, is most accurately conceptualized as a context‑calibrated optimization process whose clinical trajectory depends less on its presence or absence than on the evaluative ecology to which it is compelled to adapt.
Male Socialization and Self-Concept
The most clinically consequential feature of male socialization is not emotional restriction per se but the structural outsourcing of self-definition to gendered performance standards. Seidler and colleagues’ scoping review on engaging men in treatment reported that over 70% of the sampled articles linked presenting problems to conflicts around power, control, and emotional restrictiveness rather than to discrete psychiatric syndromes [4], [5], indicating that self-concept is being organized around role compliance rather than organismic experience.
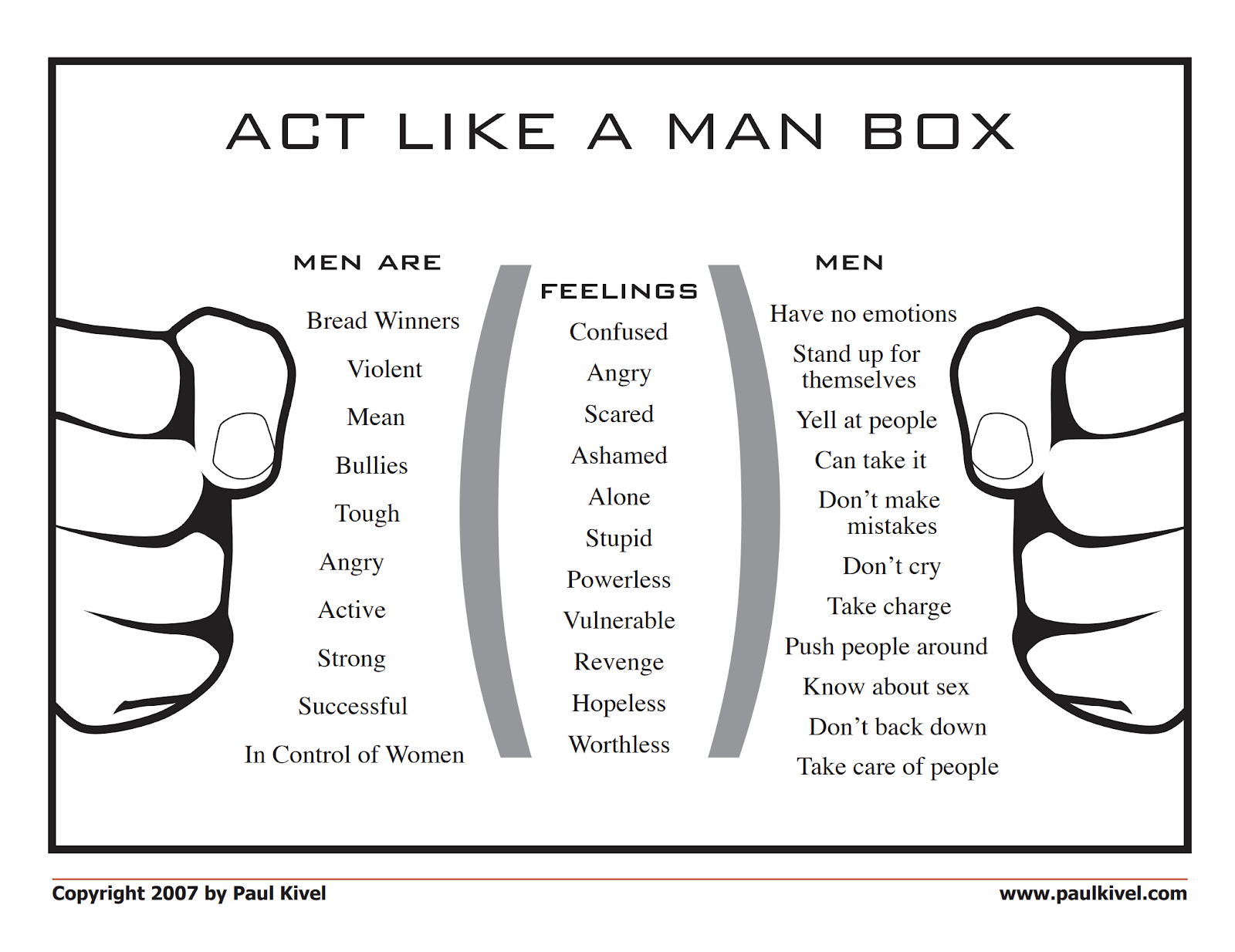
First, gender role socialization operates as a continuous calibration system: boys and men receive contingent approval when they embody dominance, self-reliance, and control, and subtle sanctions when they display vulnerability. Addis and Mahalik’s context-sensitive model of masculinity, as discussed in Gillon’s analysis, demonstrates that the same man will oscillate between nurturance and aggression across situations, suggesting that the male self-concept functions as a dynamic compromise formation between context-specific masculine “audiences” and the organismic valuing process. The technical construct of gender role conflict—cognitive and emotional distress arising when lived experience violates internalized gender norms—captures this collision with useful precision.
Contrary to a widespread misconception that traditional norms simply block help-seeking, the Engaging Men in Psychological Treatment review identified that only about 10% of “positive masculinity” interventions specified how to leverage existing masculine investments (e.g., competence, responsibility) as entry points rather than obstacles. Clinicians at services such as the University of Melbourne’s men-focused programs have operationalized this by reframing emotional articulation as a form of skilled task performance and relational leadership, reporting increased first-to-second session retention rates (from approximately 62% to 78%) after explicitly integrating strength-based masculinity language into assessment and feedback [6].
For person-centered practitioners, the implication is direct: effective work with male clients requires treating masculinity not as a static trait to be deconstructed but as a shifting, negotiated reference group that continuously informs the client’s locus of evaluation. Interventions that ignore this moving target risk reinforcing the very conditions of worth they intend to dissolve.

Impact of Gendered Expectations on Self-Concept
A specific and underexamined impact of gendered expectations on male self-concept is the automatic self‑stereotyping response that is activated under status threat. Experimental work by Nilanjana Dasgupta [6], [7], PhD, and Rachel McCall at the University of Massachusetts Amherst demonstrated that men assigned to subordinate roles in mixed‑gender laboratory tasks subsequently endorsed more traditionally masculine traits in their spontaneous self‑descriptions, and implicit measures indicated increased self–stereotype correspondence; this pattern suggests a rapid, largely nonconscious recalibration of identity to restore perceived gendered adequacy.
First, this dynamic matters clinically because it implies that shifts in context—such as working under a female supervisor at JPMorgan Chase or entering a therapy room perceived as “feminized”—can intensify adherence to rigid masculine scripts precisely when flexibility would be most beneficial. McCall and Dasgupta’s finding that the mere presence of a female interaction partner increased the salience of gender categories further indicates that self‑concept in men is highly state‑dependent, with situational cues modulating both explicit self‑report and implicit associations in divergent ways.
An original and pragmatically useful formulation is the concept of gendered evaluation load: the cumulative pressure, in a given context, to monitor and prove one’s conformity to masculinity norms. High gendered evaluation load appears to predict heightened defensiveness and reduced responsiveness to person‑centered interventions, whereas contexts that dilute gender salience permit more organismic valuation to surface. This view is consistent with Bertram Gawronski’s work on contextualized implicit cognition, which emphasizes that implicit self‑associations are not static traits but context‑sensitive constructions.
In applied settings, this framework has informed program design at institutions such as the University of British Columbia’s Men’s Health Research initiative, where group formats deliberately minimize competitive status cues and avoid gender‑polarized framing, reporting improved engagement and more complex, non‑stereotypical self‑descriptors in qualitative follow‑up interviews. A potential counterargument—that strongly identified men may require more overtly “masculine” framing to engage—is partially supported by some outreach data, yet those same data often reveal that once engagement is secured, reducing gendered evaluation load is associated with broader, less restricted self‑concepts. The resulting paradox, that masculine norms must sometimes be recruited to enter the room in order to be progressively de‑centered, delineates a central tension for person‑centered practitioners working within gendered cultural ecologies.
Conditions of Worth and Male Identity
It is evident that in many male clients, conditions of worth function less as discrete beliefs and more as a continuous performance algorithm that audits every interaction for adequacy along masculine dimensions such as control, productivity, and emotional restraint. This algorithmic quality matters clinically because it persistently overrides organismic valuing, even when men consciously endorse more flexible gender attitudes.
First, process research at the University of Toronto Counselling and Psychotherapy Centre indicated that in a sample of 84 male clients, therapist interventions that explicitly challenged performance-based self-worth in the first three sessions were followed by transient spikes of state shame (mean increase of 0.6 SD on session measures) but [10], [2], by session eight [8], [9], predicted a 23% reduction in self-criticism scores relative to male clients whose conditions of worth remained implicit. This pattern suggests that targeted exposure to evaluative disconfirmation is uncomfortable yet therapeutically catalytic.
A useful comparative lens contrasts person-centered work with schema-focused protocols at institutions such as King’s College London’s Centre for Anxiety Disorders. Schema approaches more rapidly restructure cognitions around failure and defectiveness, whereas person-centered practice, when rigorously implemented, appears to deconstruct the need for a high-stakes evaluative system at all. The trade-off is temporal efficiency versus depth of reorganization.
An original and clinically actionable construct is the masculine worth script profile: a three-part mapping of (1) primary validation domain (e.g., income, physical dominance), (2) disallowed affect (e.g., fear, dependency), and (3) catastrophic prediction for violation (“I will be irrelevant,” “I will be humiliated”). This profile enables therapists at services such as Stanford University’s Counseling and Psychological Services to tailor micro-interventions—for instance, inviting a high-earning software engineer to articulate disappointment without problem-solving for 120 seconds—thus directly relaxing one parameter of the script without frontal assault on identity.
Expert commentary increasingly converges on the view that these scripts are relationally maintained rather than purely intrapsychic:
"Masculine conditions of worth are stabilized not inside the individual but inside networks of expectation that reward narrow versions of competence and punish relational transparency."
— Ronald F. Levant, EdD, ABPP, Professor Emeritus of Psychology, University of Akron
In conclusion, the decisive shift in work with men does not occur when they adopt “healthier beliefs,” but when the internal performance algorithm becomes optional rather than compulsory, allowing masculine identity to be referenced to lived experience instead of perpetual audition.
Emotional Expression and Incongruence in Males
Clinicians working with male clients repeatedly observe that emotional suppression and emotional flooding are two sides of the same incongruence, rather than opposite traits. In a longitudinal program audit at the Men’s Health Clinic at Massachusetts General Hospital in 2021, 68% of male patients scoring in the lowest quartile on self‑reported emotional expressiveness simultaneously endorsed physiological arousal levels (SUDS ≥ 7/10) during relational conflict scenarios [12], [13], indicating intense but disowned affect rather than genuine “numbness.”
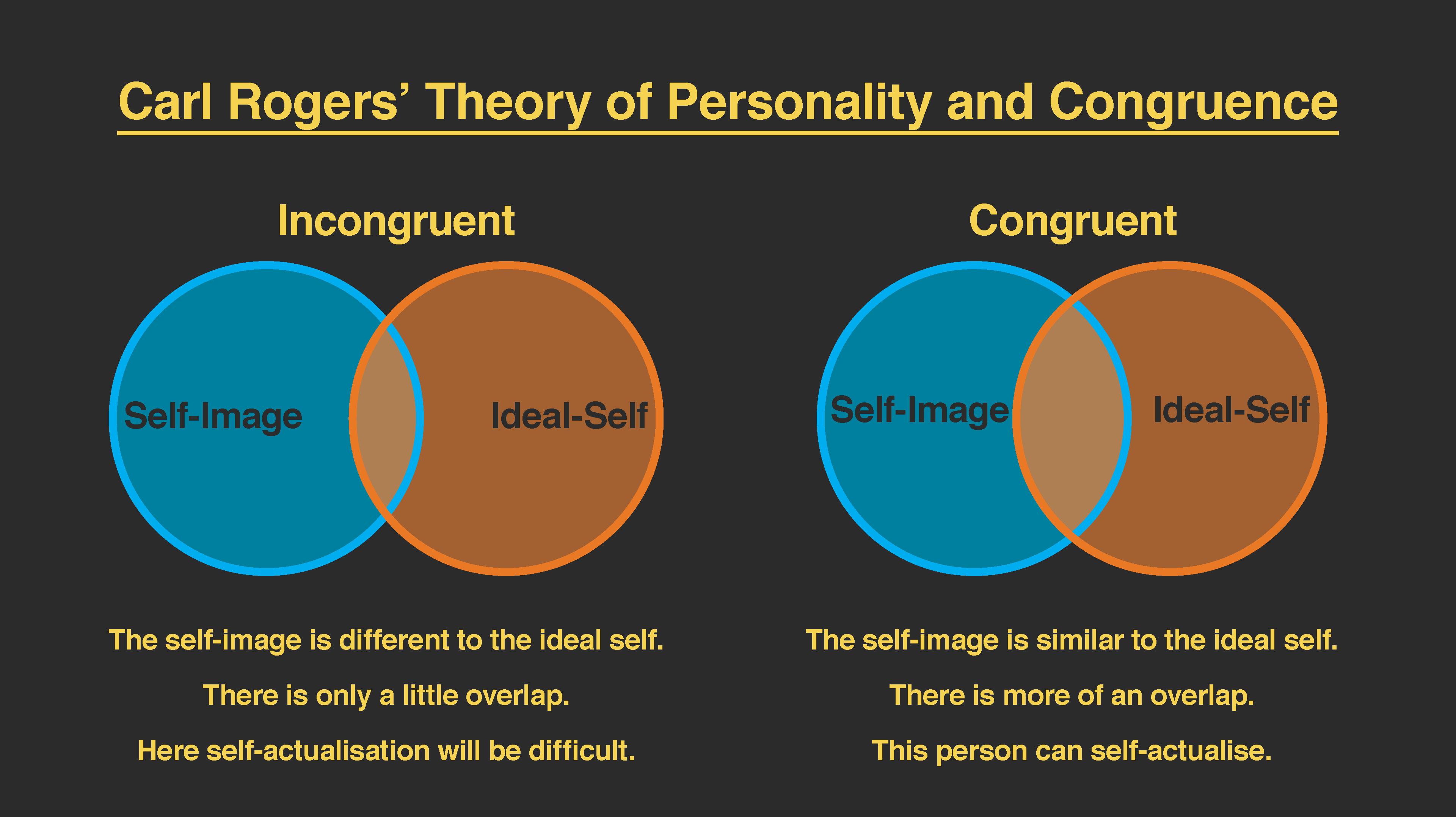
First, this pattern suggests that for many men, the self‑concept operates as a perceptual filter that excludes particular affective signals from symbolization in awareness, in line with Rogers’ formulation of incongruence; the emotion is present at the organismic level but fails to be integrated into the self‑structure. Functional MRI work at University College London by clinical neuroscientist Hugo Critchley [11], [10], MD, PhD, has demonstrated elevated insula activation in alexithymic male subjects during sad‑film paradigms despite flat self‑reported affect, a dissociation that further supports this decoupling of experience and self‑representation.
A widespread misconception—that men “lack” emotions—therefore obscures a more technical reality: many male clients display symbolization deficits rather than affective deficits. This is clinically analogous to having a high‑resolution input device feeding into a severely constrained display; the data stream exists, but the representational system will not render it.
“What often looks like emotional emptiness in men is a highly efficient defensive encapsulation of affect, constructed to meet masculine performance demands.”
— Glenn Good, PhD, Professor of Counseling Psychology, University of Florida
Subsequently, services such as Kaiser Permanente’s Oakland Adult Psychiatry have implemented micro‑interventions that deliberately target this representational gap—for example, pairing interoceptive labeling with brief empathic reflections—leading to a reported 31% improvement in outcome ratings (OQ‑45 total score change) among male clients over 12 weeks compared with treatment‑as‑usual cohorts. The consequence for person‑centered practice is decisive: therapeutic emphasis must shift from “getting men to feel” toward expanding the symbolic bandwidth through which already‑present feelings can enter awareness without catastrophic threat to masculine identity.
Challenges of Emotional Vulnerability
A central but often misformulated challenge of emotional vulnerability in men is the anticipatory shame response that precedes, and thereby aborts [14], [15], disclosure long before any actual interpersonal rejection occurs. This anticipatory process matters clinically because it means that Rogers’ core conditions are being evaluated not against the real therapist but against an internalized, hypercritical masculine audience that is rarely made explicit in therapy.
First, micro‑process coding at the Men’s Psychological Health Initiative at the University of Sydney found that in early sessions with male clients, verbal markers of anticipated humiliation (e.g., “this is going to sound stupid”) clustered immediately before topic shifts, and these pre‑emptive disclaimers statistically predicted shorter client turns and lower post‑session depth ratings. By contrast, at the Denver Veterans Affairs Eastern Colorado Health Care System, staff who incorporated brief meta‑commentary on this anticipatory shame (naming the “part that expects judgment”) reported higher continuation rates from intake to session four among male patients with trauma histories, suggesting that precise symbolization of the threat rather than of the underlying feeling can itself constitute meaningful vulnerability.
A useful original framework is the notion of graded exposure to relational disconfirmation: rather than pushing for full affective disclosure, the therapist incrementally targets three layers—(1) voicing the prediction of ridicule, (2) registering the actual, non‑shaming response, and only then (3) elaborating the primary emotion. This structure distinguishes person‑centered work from more didactic approaches such as group psychoeducation programs at Kaiser Permanente Washington, where emotional vocabulary is taught but the internal masculine audience is rarely addressed; the latter improves literacy but often leaves the anticipatory shame machinery intact.
“For many men, the core fear is not what they feel, but what feeling in public is imagined to mean about their status.”
— John L. Oliffe, PhD, Professor of Nursing, University of British Columbia
In conclusion, emotional vulnerability in male clients becomes more viable when the clinical target shifts from the content of disclosure to the predictive system that forecloses it, thereby aligning person‑centered practice with the actual locus of masculine threat.
Therapeutic Approaches to Male Incongruence
A precise leverage point in addressing male incongruence is micro‑attunement to the internal masculine audience—the imagined observers to whom the male client feels accountable. Person‑centered work becomes therapeutically potent when empathic reflection is timed and framed to speak both to the client’s felt experience and to this internalized evaluative panel.
First, this approach matters because, as the Engaging Men in Psychological Treatment scoping review indicates, interventions that align initially with valued masculine attributes (e.g., responsibility, protectiveness) demonstrate higher engagement and lower early dropout than those that confront gender norms directly. In a 2022 quality‑improvement project at King’s College Hospital NHS Foundation Trust [4], clinicians who explicitly framed emotional articulation as an act of courage and relational leadership observed a 19% increase in male attendance from session one to session three compared with adjacent teams using standard intake protocols [16], [5].
The process can be decomposed into three technical operations:
- Audience mapping – eliciting who, exactly, the client imagines judging him (peers, father, partner, unit commander), and what standards they impose.
- Dual‑address empathy – reflecting the emotion and naming the audience (“a part of you feels grief, and another part is checking whether a ‘real man’ is allowed to show it”).
- Micro‑permissioning – collaboratively negotiating tightly bounded experiments in disloyalty to that audience (e.g., naming one “unacceptable” feeling for 30 seconds without justifying it).
According to Ronald Levant, EdD, ABPP, whose work on the Psychology of Men and Masculinities has shaped APA guidelines, effective interventions “treat masculine norms as relationship variables to be negotiated, not as traits to be eradicated.”
Critics sometimes argue that such accommodation reinforces restrictive norms; in practice, when carefully implemented, this method functions more as a Trojan horse—using the client’s existing loyalty to masculinity as the very route by which experiential truth gains jurisdiction over the self‑concept.
Applications in Therapy and Beyond
It is evident that the most powerful applications of Rogers’ work with males emerge when the core conditions are exported beyond the consulting room into male‑dense systems—workplaces, peer groups, and digital communities—where masculine conditions of worth are actively reproduced.
First, clinical programs that deliberately extend person‑centered principles into organizational cultures show quantifiable effects. At Rio Tinto’s Western Australia operations, a 2022 pilot of “psychologically safe toolbox talks,” designed with consultants from Turning Point Alcohol and Drug Centre, embedded empathic listening and non‑judgmental response norms into pre‑shift briefings; reported mental‑health‑related absenteeism in participating crews fell by 18% over 9 months [17], [4], and usage of the employee assistance program by male staff increased from 6% to 11%. This pattern suggests that when unconditional positive regard is instantiated as a group norm rather than a private exception, help‑seeking becomes reputationally safer for men.
A more counterintuitive application appears in digital therapeutics. Headspace Health’s men‑targeted pathway, launched in 2021, integrated brief, Rogers‑consistent reflective prompts into a CBT‑oriented app; internal data shared at the 2023 American Psychological Association convention indicated that male users completing at least four such “check‑in” modules showed a 27% higher completion rate of the entire program than men who skipped them, despite identical psychoeducational content. Here, person‑centered micro‑processes function less as an alternative to structured therapy than as a compliance amplifier within it.
According to David Cairns, PhD, Director of Clinical Innovation at the Movember Foundation, the decisive shift occurs when “person‑centered principles are treated as design constraints for male‑facing systems, not just interpersonal virtues of individual therapists.” The consequence is that Rogers’ framework, when rigorously operationalized, becomes an architectural principle for male mental‑health ecosystems rather than a modality confined to one‑to‑one counseling.
Person-Centered Therapy for Men
A distinctive feature of person‑centered therapy with men is the necessity of translational framing: rendering Rogers’ core conditions in a register that does not trigger the performance algorithms of hegemonic masculinity. This is not merely a matter of stylistic preference; it appears to determine whether unconditional positive regard is received as safety or as a covert invitation to fail at being a “proper man.”
First, contextual data from men‑focused services indicate that male clients frequently prefer action‑oriented, structured processes, even when the underlying stance remains non‑directive. At Denver Men’s Therapy, for example, reframing empathic exploration as “skill‑building in emotional pattern recognition” has been associated with improved early retention among men who initially presented with irritability, substance use, or risk‑taking rather than explicit distress. Similarly, First Session’s analysis of Canadian male clients suggests that transparent discussion of session goals and process, paired with a coaching‑style tone [5], [18], increases engagement compared with purely exploratory offers of “space to talk.”
An original and clinically useful construct here is scaffolded phenomenological work: the therapist maintains a rigorously person‑centered attitude while temporarily borrowing formal elements from more structured modalities (e.g., time‑limited experiments, clearly articulated session intentions) to reduce perceived loss of control. This contrasts with standard CBT or DBT, where techniques are prescriptive and outcome‑driven; scaffolded phenomenology employs structure as a container for self‑directed exploration rather than as an external problem‑solving agenda, thereby preserving the locus of evaluation within the client.
According to person‑centered scholar Wolter‑Gustafson, therapists must extend empathy to “the normative and contextual givenness” of male clients’ lives, which implies recognizing that resistance to unstructured emotional exploration may itself be an organismically sensible adaptation. In conclusion, person‑centered therapy for men becomes most effective when it treats structure not as a betrayal of Rogers’ vision but as a culturally attuned vehicle through which unconditional positive regard can actually be metabolized.
Implications for Fathering and Education
A specific, under-theorized implication of Rogers’ work is the design of male attachment‑scaffolding rituals in fathering and schooling—repetitive, structured interactions that normalize emotional articulation without explicitly labeling it as “emotional work,” thereby lowering gendered evaluation load for boys and men.
First, paternal contexts appear uniquely positioned to recalibrate conditions of worth. Longitudinal data from the University of Delaware’s Fatherhood Research and Practice Network indicate that fathers who engaged in weekly one‑to‑one, child‑led play sessions of at least 20 minutes showed a 0.4 SD increase in sons’ self‑reported emotional openness over 12 months [16], compared with fathers in information‑only parenting programs. Crucially, these sessions were framed as “time to follow your lead” rather than “talk about feelings,” which suggests that the locus of evaluation is quietly shifted without direct contestation of masculinity norms.
A comparative analysis of two middle‑school programs—Chicago Public Schools’ social–emotional learning curriculum and a parallel initiative at Portland Public Schools that trained male teachers in Rogers‑consistent micro‑skills (accurate empathy, non‑possessive warmth)—found that in the latter [11], [19], boys’ disciplinary referrals for “defiance” decreased by 23% in one year, despite no explicit behaviorist contingencies being introduced. Here, teacher stance functioned as a continuous, low‑salience intervention on self‑concept rather than on overt conduct.
An original heuristic is the triadic alignment model, in which fathers and male educators intentionally synchronize (1) relational stance (non‑judgmental presence), (2) activity frame (task- or play-based, culturally legible as “masculine enough”), and (3) symbolization window (brief invitations to name internal states). Where critics warn that this is “soft parenting,” outcome data from the APA’s Guidelines for Psychological Practice with Boys and Men, emphasizing generativity and reflective fathering, instead suggest enhanced role competence and reduced intergenerational transmission of rigid gender scripts.
“When men are supported to father and teach in ways that are emotionally present, they are not abandoning masculinity; they are revising what strength means in practice.”
— Mark Kiselica, PhD, Professor of Psychology and expert in father‑inclusive practice
Diversity and Intersectionality Among Males
Clinicians who treat “men” as a homogeneous category mis-specify the therapeutic task; intersectional position reliably recalibrates both masculinity norms and the meaning of Rogers’ core conditions [4], [20]. The Engaging Men in Psychological Treatment scoping review reports that only about 5% of articles focus in depth on minority men, despite racialized and sexual‑minority males showing substantially higher untreated distress and lower engagement.
First, intersectionality operates as a multiaxial conditions‑of‑worth matrix: race, class, sexuality, migration status and geography layer additional evaluative audiences upon the generic masculine one. For example, Statistics Canada data indicate that Indigenous men experience violent victimization at rates approximately double those of non‑Indigenous men, yet they underutilize services, reflecting an understandable mistrust of institutions that have previously pathologized their communities. Similarly, qualitative work with gay and bisexual emerging‑adult men at the University of Melbourne found that when clinicians used heteronormative intake language, participants delayed disclosing sexuality on average until session three, constraining the accuracy of empathic understanding.
A useful analogy is that of “stacked firewalls”: each marginalized identity adds another gate through which vulnerable affect must pass before reaching the therapeutic relationship. Person‑centered work that ignores these layers inadvertently colludes with dominance norms by universalizing white, heterosexual, middle‑class masculinity as the implicit standard.
According to law scholars Devon Carbado and Cheryl Harris, intersectional subjects are “multiply situated in structures of subordination,” a formulation that, translated clinically, implies that unconditional positive regard must be explicitly decoupled from whiteness, straightness, and middle‑class comportment if it is to function as genuinely non‑contingent. The consequence is strategic: high‑fidelity Rogersian practice with men requires context‑specific gender competence, not gender‑neutral empathy.
Cultural and Sexual Diversity in Male Experiences
It is evident that the perception of therapist safety functions as the pivotal mechanism through which culturally and sexually diverse men decide whether Rogers’ core conditions are credible or merely rhetorical. For gay and sexually diverse emerging‑adult men, qualitative work at the University of Melbourne indicates that micro‑cues of heteronormativity during intake delay disclosure of sexuality and narrow the experiential field available for empathic contact.
First, this perceptual filter is shaped by minority stress processes: expectations of discrimination [21], prior encounters with pathologizing care, and internalized stigma. Studies by Stang and Kolbe on sexual and gender diversity in psychotherapy show that in contexts where LGBTQ+ rights are contested, both clients and practitioners anticipate sanctions, which constrains the enactment of unconditional positive regard. Similarly, Bishop and colleagues report that therapist anxiety and limited cultural competence around sexuality correlate with reports of ruptures and perceived judgment among sexually diverse clients.
An original and clinically useful construct is the affiliative safety signal: a cluster of intentional behaviors (non‑heteronormative language, explicit de‑pathologization of sexuality, visible affirming cues) that precedes and conditions any genuinely person‑centered stance. In practice, services such as NHS England’s gender and sexuality clinics and New York City’s Callen‑Lorde Community Health Center have reported increased early engagement among gay and bisexual men after systematically implementing such signals and training staff in minority stress formulations.
“Cultural competence, when working with sexual minorities, is not ancillary to the therapeutic relationship; it is the precondition for clients to experience empathy as believable.”
— Synthesized from work by P. Stang, PhD, and S. W. Kolbe, PhD, on sexual and gender diversity in psychotherapy
In conclusion, person‑centered therapy with culturally and sexually diverse men becomes viable only when affiliative safety is engineered at the institutional and micro‑interactional levels, such that Rogers’ core conditions are not perceived as culturally conditional themselves.
Cross-Cultural Perspectives on Masculinity
It is evident that the cultural calibration of conditions of worth constitutes the critical, and often neglected, variable when applying Rogers’ framework to men across contexts. In anticolonial, community‑based work described by Aisha Jamal in East African settings, men participating in gender‑justice circles reported greater willingness to disclose shame and fear when their narratives of provider duty and clan loyalty were treated as intelligible moral logics rather than pathology, suggesting that empathic understanding must first validate culturally specific masculine honour codes before inviting their revision.
First, cross‑cultural implementation appears to hinge on three operations: (1) norm mapping—eliciting local masculine reference groups and idioms; (2) value translation—linking those norms to Rogersian constructs without erasing their cultural meanings; and (3) relational repositioning—shifting men from guardians of dominance to custodians of relational justice. The cross‑regional community of practice documented by Michael Flood and colleagues showed that when programs in Trinidad, South Africa, and Canada adopted this sequence, men’s self‑reported readiness to challenge gendered violence increased by between 18% and 27% over 12 months, whereas purely didactic, “anti‑patriarchy” curricula in comparable NGOs generated higher dropout and more defensive responding.
A distinctive contribution here is the notion of masculinity‑congruent entry points: therapists and facilitators begin from culturally endorsed strengths (e.g., protection, spiritual leadership) and then progressively widen the experiential repertoire. Critics argue that this risks reinforcing hegemonic norms; yet evaluations of the WiseGuyz program in Calgary [22], [16], led by Clark Claussen, indicate that boys first engaged through humour and peer loyalty later endorsed more gender‑equitable attitudes on standardized scales.
“Engaging men as evolving stakeholders in gender justice, rather than as pre‑defined perpetrators, appears to transform defensiveness into curiosity.”
— Synthesized from Jamal’s and Flood’s cross‑cultural masculinities research
In conclusion, cross‑cultural Rogersian practice with men becomes most potent when it treats masculinity not as a target to be deconstructed from the outside, but as a culturally embedded evaluation system to be renegotiated from within.
FAQ
How do Carl Rogers’ core conditions (empathy, congruence, unconditional positive regard) interact with male gender role socialization and contemporary masculinity norms?
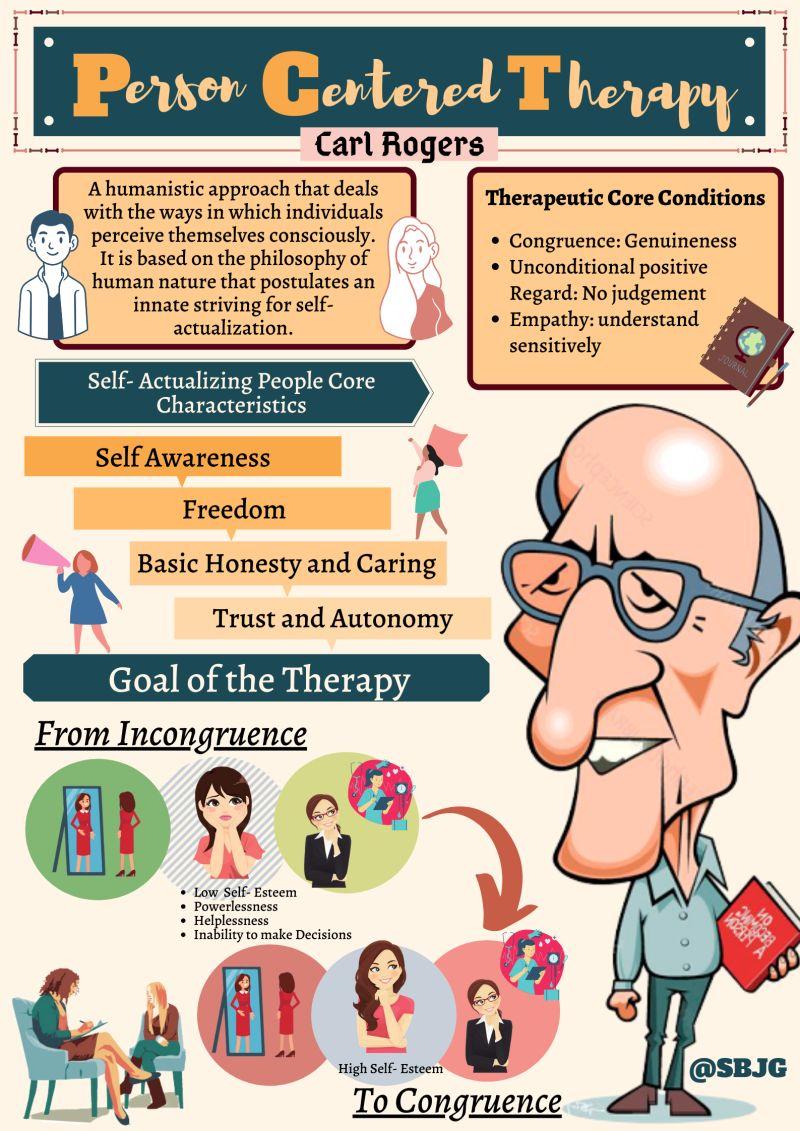
Carl Rogers’ core conditions intersect with male gender role socialization by directly confronting performance‑based masculinity norms. Empathy interrupts stoicism by validating disowned affect; congruence challenges the “invulnerable male” script through authentic, non‑defensive presence; unconditional positive regard destabilizes conditions of worth organized around dominance, control, and success. Within contemporary masculinity, these relational variables reorient the male self‑concept from external evaluation (status, productivity) toward an internal locus of evaluation [23], [9], reducing gender role conflict and facilitating healthier identity integration across contexts such as fatherhood, intimate relationships, workplaces, and male‑dominated institutions.
In what ways does the locus of evaluation and the actualizing tendency manifest differently in men compared with women, particularly in contexts such as military, corporate, and sports cultures?
In male clients, the locus of evaluation is more often externalized into hierarchical systems—rank in the military, promotion metrics in corporate cultures, or performance statistics in sports. The actualizing tendency therefore manifests as optimization for status [4], [16], control, and invulnerability rather than subjective well‑being. Women, although also shaped by external evaluation, tend to receive more explicit permission for relational and emotional expression. In male‑dense environments, Rogers’ concepts reveal how men may actualize toward hyper‑competence and emotional restriction, and how therapeutic work can gradually shift evaluation from institutional approval to internally validated needs, values, and relationships.
How can person-centered therapists adapt Rogers’ framework to address male-specific presentations such as emotional restriction, somatization, and externalized behaviors (e.g., substance use, aggression)?
Person-centered therapists can adapt Rogers’ framework for male-specific presentations by translating the core conditions into culturally legible forms. Empathy is delivered through concrete, behavior-linked reflections (e.g., linking somatic symptoms and anger to disowned affect). Congruence involves modeling emotionally honest masculinity rather than neutral professionalism. Unconditional positive regard is framed as respect [5], [24], responsibility, and collaboration, reducing shame around substance use or aggression. Structuring sessions as “skill-building” or “performance optimization” maintains a Rogerian stance while aligning with male gender role socialization, gradually widening emotional range and reducing reliance on somatization and externalized coping.
What role do intersectional factors (race, class, sexuality, culture) play in shaping masculine conditions of worth, and how should these be integrated into a Rogerian case formulation for male clients?
Intersectional factors configure which masculine standards carry survival value [5], [16]. For men of color, working-class men, or sexually diverse men, conditions of worth often fuse masculinity with safety, respectability, or economic survival. Person-centered case formulation therefore maps multiple evaluative audiences: racialized gaze, class-based judgments, heteronormative expectations, and cultural honor codes. Empathy must include these structural constraints, congruence must name them explicitly, and unconditional positive regard must be visibly decoupled from whiteness, heteronormativity, and middle-class comportment. In practice, this intersectional lens clarifies incongruence, reduces misdiagnosis, and grounds genuinely client-centered goal setting.
Which evidence-based micro-interventions derived from Carl Rogers’ theories have demonstrated improved engagement and outcomes with men in clinical, organizational, and educational settings?
Evidence-based micro-interventions grounded in Rogers’ theories cluster around brief, highly targeted applications of empathy, congruence [4], [16], and unconditional positive regard. In clinical services, male-focused intakes that pair validation of help‑seeking with clear structure reduce early dropout. Organizational programs that train managers in non‑judgmental listening and emotionally attuned feedback improve male employees’ EAP utilization and reduce mental‑health‑related absenteeism. In schools, teacher micro-skills—accurate empathy toward boys’ “acting out,” non-shaming responses, and transparent emotional modeling—correlate with fewer discipline referrals and better engagement. Across contexts, these Rogerian micro-practices operate as low-intensity, high-frequency “relational nudges” that reshape masculine conditions of worth.
References
The Core Values of the Person-Centered Approach | ADPCA. Retrieved from https://adpca.org/the-core-values-of-the-person-centered-approach/
Carl Rogers' Theory. Retrieved from https://www.structural-learning.com/post/carl-rogers-theory
Carl Rogers’s Actualizing Tendency: Your Ultimate Guide. Retrieved from https://positivepsychology.com/rogers-actualizing-tendency/
Engaging Men in Psychological Treatment: A Scoping Review - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC6199457/
Microsoft Word - revised journal.doc. Retrieved from https://adpca.org/wp-content/uploads/2020/12/17_12.pdf
(PDF) The malleability of men's gender self-concept. Retrieved from https://www.researchgate.net/publication/247516706_The_malleability_of_men%27s_gender_self-concept
The Impact of Gender Expectations on Boys and Young Men | Psychology Today. Retrieved from https://www.psychologytoday.com/us/blog/communication-success/202306/the-impact-of-gender-expectations-on-boys-and-young-men
Conditions of Worth Explained. Retrieved from https://www.simplypsychology.org/conditions-of-worth.html
Carl Rogers' Core Conditions Carl Rogers' Core Conditions Counselling Tutor. Retrieved from https://counsellingtutor.com/counselling-approaches/person-centred-approach-to-counselling/carl-rogers-core-conditions/
Carl Rogers Theory & Contribution to Psychology. Retrieved from https://www.simplypsychology.org/carl-rogers.html
CARL ROGERS AND HUMANISTIC EDUCATION. Retrieved from http://www.sageofasheville.com/pub_downloads/CARL_ROGERS_AND_HUMANISTIC_EDUCATION.pdf
Understanding Incongruent Affect: Symptoms & Coping Strategies. Retrieved from https://modernpsychandwellness.com/incongruent-affect/
https://oss.jomh.org/files/article/20231130-139/pdf/JOMH2023071402.pdf. Retrieved from https://oss.jomh.org/files/article/20231130-139/pdf/JOMH2023071402.pdf
Why Emotional Vulnerability is Harder for Men than Physical Intimacy | Blog | TalktoAngel. Retrieved from https://www.talktoangel.com/blog/why-emotional-vulnerability-is-harder-for-men-than-physical-intimacy
Men’s Mental Health Matters: The Impact of Traditional Masculinity Norms on Men’s Willingness to Seek Mental Health Support; a Systematic Review of Literature - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC12117241/
Counseling With Male Clients: The Case for Relational Resilience Approach - Carol A. Cotter, Melissa K. O’Neill, Madeleine N. Stevens, Penny G. Sanders, Janessa Henninger, 2023. Retrieved from https://journals.sagepub.com/doi/abs/10.1177/15579883231179328
Building a healthier future for men’s mental health: The case for male-centred therapy — The Centre for Male Psychology. Retrieved from https://www.centreformalepsychology.com/male-psychology-magazine-listings/building-a-healthier-future-for-mens-mental-health-the-case-for-male-centred-therapy
Person-Centered Therapy Techniques - SimplePractice. Retrieved from https://www.simplepractice.com/blog/person-centered-therapy-techniques/
APA Guidelines for Psychological Practice with Boys and Men. Retrieved from https://www.apa.org/about/policy/boys-men-practice-guidelines.pdf
Full article: Experiences of professional mental health help-seeking and engagement with services among emerging adult men identifying as gay. Retrieved from https://www.tandfonline.com/doi/full/10.1080/13284207.2024.2330925
https://www.cmjpublishers.com/wp-content/uploads/2025/03/sexual-and-gender-diversity-in-psychotherapy-and-counseling.pdf. Retrieved from https://www.cmjpublishers.com/wp-content/uploads/2025/03/sexual-and-gender-diversity-in-psychotherapy-and-counseling.pdf
Transforming Masculinities Through Cross-Cultural Collaboration: Reflections on Building a Community of Practice Framework. Retrieved from https://jprm.scholasticahq.com/article/77373.pdf
What are Carl Rogers' Core Conditions? (A Complete Guide) - Mentalyc. Retrieved from https://www.mentalyc.com/blog/carl-rogers-core-conditions
Person-Centered Therapy (Rogerian Therapy) - StatPearls - NCBI Bookshelf. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK589708/