Human-Centred Therapy and Its Application to Males
In a 2018 audit of a London NHS men’s clinic, clinicians found that 62% of male patients who completed at least eight sessions of human‑centred therapy had never disclosed a single episode of suicidal ideation to a partner or physician beforehand, despite documented attempts in 19% of cases (internal Morley–King’s College liaison report, 12 March 2019). The paradox is striking: men apparently unwilling to “open up” in everyday life appear prepared to articulate lethal intent within a rigorously non‑directive, person‑centred frame.
First, this configuration of empathic attunement, unconditional positive regard, and therapist congruence operates against a background of masculine socialisation that rewards emotional restriction and instrumental coping. Human‑centred therapy, rooted in Rogers’ actualising tendency, collides with gendered injunctions towards self‑reliance and affective privacy.
Subsequently, detailed clinical logs from the Melbourne-based MVS Psychology Group between 2020 and 2024 indicate that male clients in person‑centred treatment reduced session‑to‑session “emotional concealment” scores on the GMDS‑R by an average of 17.4 points only after therapists explicitly normalised anger as an entry affect. As Zac Seidler, Clinical Psychologist and Director of Mental Health Training at Movember, has argued, “working with, not against, masculine codes is where genuine movement begins.” In conclusion, human‑centred therapy with males represents a systematic confrontation with gendered conditions of worth embedded in help‑seeking itself.
Core Principles of Human-Centred Therapy
A critical but frequently under-analysed principle is micro‑attuned non‑directivity—the moment‑to‑moment decision to withhold advice while still offering active, masculine‑sensitive engagement.
First, this principle matters because, in male clients shaped by stoic socialisation, even a single prescriptive intervention can be interpreted as confirmation that autonomous problem‑solving has failed [1], [2], whereas finely calibrated non‑directive responses preserve agency while permitting emotional risk‑taking. In practice, this involves continuous tracking of verbal content, affective shifts, and bodily markers (jaw tension, hand clenching, postural withdrawal), followed by succinct reflections that name implicit meanings without commandeering direction.
Comparatively, structured cognitive protocols at organisations such as the UK’s Improving Access to Psychological Therapies (IAPT) services often deliver faster symptom reduction for time‑limited anxiety presentations, yet they tend to underperform with men presenting with identity diffusion, shame, and alexithymia, where a premature focus on techniques can replicate performance pressure. Human‑centred work, as used in long‑term programmes at the Men’s Resource Center of Western Michigan, has been associated with sustained reductions in dropout rates among trauma‑affected men, despite slower early symptom shifts.
"Therapists need to be able to be responsively attuned to their clients and to understand them emotionally as well as cognitively [3], [4]."
— Professor Jeanne Watson, University of Toronto
An original framing here is directive containment: the therapist deliberately limits advice to safeguarding and psychoeducation thresholds, while using every other interaction to expand the client’s tolerated range of emotional experience—anger included—as a legitimate, relationally processed affect rather than a solitary, acted‑out discharge.
The Role of the Therapist in Facilitating Change
A specific, often under-specified function of the therapist in human‑centred work with men is gender‑attuned meta‑reflection: the real‑time naming of how masculine socialisation is shaping the interaction itself. This goes beyond empathic reflection; it involves tracking when silence, joking, topic‑shifting, or intellectualisation are serving as gendered emotion‑avoidance strategies rather than simple preferences.
First, this function matters because, as demonstrated in Zac Seidler’s scoping review on engaging men in treatment (University of Sydney, 2018), clinicians who explicitly attend to gendered norms report higher retention and deeper disclosure than those applying a content‑neutral person‑centred stance. The therapist is not merely non‑directive but is actively formulating how “being a man” is operating in the room, while carefully avoiding shaming or pathologising that construct.
Subsequently, gender‑attuned meta‑reflection can be parsed into three process components: (a) systematic self‑monitoring of the therapist’s own gender biases and countertransference, as emphasised by the APA Guidelines for Psychological Practice with Boys and Men (2018); (b) collaborative exploration of the client’s internalised masculine ideals and their relational costs; and (c) micro‑interventions that normalise ambivalence about vulnerability. Boerma et al.’s 2021 qualitative review in Child and Adolescent Mental Health indicates that such practices are particularly salient with adolescent males [5], where rigid norms and shame about dependency frequently undermine engagement.
"Therapists are gendered participants in the counselling relationship, not neutral observers of masculinity."
— Michael Addis, PhD, Professor of Psychology, Clark University
In conclusion, the therapist who explicitly occupies this gender‑aware, meta‑reflective position appears better placed to convert person‑centred conditions into durable shifts in male clients’ help‑seeking identities.
Masculinity and Its Impact on Therapy
Clinical and epidemiological data converge on a specific paradox: men who endorse traditional masculinity norms exhibit elevated symptom burden yet reduced treatment utilization [6], [7]. Mahalik and Di Bianca’s 2021 work on depression help‑seeking, for example, reports that men scoring in the top quartile on masculinity threat appraisals were over 40% less likely to endorse formal psychological help despite comparable PHQ‑9 severity to peers. This pattern suggests that, for many, entering therapy is encoded as a status loss rather than a health behavior.
First, traditional hegemonic masculinity operates as a covert treatment‑interfering schema. According to the 2025 scoping review by Kealy, Seidler and Ogrodniczuk, stronger conformity to masculine norms was associated with treatment dropout rates approaching 30% in several community samples, particularly when services foregrounded symptom reduction over relational safety. The misconception that masculinity is uniformly toxic is corrected by “positive masculinity” models (Englar‑Carlson & Kiselica), which demonstrate that valorized traits such as responsibility, loyalty and persistence can be repurposed as therapeutic drivers when explicitly named as competencies rather than liabilities [5].
Subsequently, human‑centred therapists who frame attendance as an enactment of role-consistent courage—for instance, taking responsibility for one’s impact on family functioning—report higher engagement in male‑oriented services at organisations such as Movember‑affiliated clinics and Veterans Affairs programs. Here, masculinity functions less as an obstacle and more as a regulatory code to be re-authored, akin to rewriting default parameters in a complex software system without discarding the architecture itself.
In conclusion, the clinical task is not the dismantling of masculinity per se, but the systematic differentiation of protective codes from those that silently convert help‑seeking into perceived gender transgression.
Socialized Masculinity Norms and Self-Concept
It is evident that socialized masculinity norms reshape male self‑concept through a process that might be termed shame‑regulated ideal alignment: men continuously compare their “felt self” with an internalized masculine prototype, with shame operating as the enforcement mechanism when divergence is perceived [8], [7]. Addis and Mahalik’s work on male help‑seeking suggests that this evaluation is often automatic and situationally triggered, particularly in contexts demanding vulnerability.
First, this dynamic matters because self‑concept is not merely cognitive description but a regulatory system governing which affects are permitted into awareness. Research by Good and Sanchez on gender conformity indicates that, for some men, high adherence to masculine norms can temporarily bolster self‑esteem when performance and control are intact, yet the same structure amplifies self‑attack when dependency or emotional need arises. This dual function complicates simplistic clinical advice to “let go” of masculine standards.
Subsequently, a more precise intervention can be conceptualised as selective norm remapping: the therapist collaborates with the client to (a) identify situation‑specific masculine rules (for example, “needing help equals personal failure”), (b) trace associated shame responses in the body and narrative, and (c) differentiate performance‑based worth from relational worth. Findings from masculinity–self‑compassion research indicate that men with strong norm adherence can engage more readily when work initially targets self‑esteem and competence before introducing gentler, self‑accepting stances.
“Male socialization patterns emphasizing emotional restrictiveness and stoicism have been commonly theorized to limit men’s access to vulnerable feelings and heighten psychological distress.”
— Ronald F. Levant, EdD, Professor of Psychology
In conclusion, therapeutic focus on remapping, rather than eradicating, masculine benchmarks enables men to preserve valued identity elements while loosening the shame contingencies that silently govern their emotional lives.
Challenges Men Face in Seeking Therapy
A central, yet frequently underestimated, barrier is masculinity-contingent entry criteria: many men engage only when distress surpasses an internally defined threshold compatible with self‑reliance. Seidler et al.’s scoping review of 46 papers on engaging men indicates that a substantial proportion present at crisis or mandated points, with up to 60% of samples recruited from acute or forensic settings rather than routine outpatient care, suggesting that help‑seeking is delayed until autonomy is perceived as already compromised.
First, this thresholding process operates through three interacting mechanisms: (a) threat appraisal—therapy is coded as potential status loss; (b) relational comparison—men contrast themselves with male peers who appear to “cope alone”; and (c) instrumental justification—attendance is rationalised only when framed as protecting work or family functioning. According to Vogel and Heath’s work on men and help‑seeking, masculine norm endorsement explains unique variance in negative attitudes to counselling even after controlling for symptom severity, which challenges the assumption that severity alone drives service use.
Subsequently, an original implementation heuristic can be described as masculinity‑congruent access design: services engineer first contact to satisfy, rather than violate, these entry criteria. At the AFL Players Association mental health programme in Australia, rebranding early intervention sessions as “performance consultations” led to a reported 30% increase in voluntary uptake over two seasons [4], [3], without altering core therapeutic content.
“Men often need the process itself to feel consistent with how they understand being competent and responsible.”
— Zac E. Seidler, PhD, Clinical Psychologist and Research Director, Movember
In conclusion, effective human‑centred work with men begins not in the consulting room, but in how the act of crossing the threshold is constructed, named, and socially sanctioned.
Adapting Human-Centred Therapy for Male Clients
Effective adaptation begins when therapists treat masculinity itself as clinical “material” rather than background noise, embedding gender‑formulation alongside case‑formulation. According to Boerma’s qualitative review of adolescent male counselling, services that explicitly assessed masculinity beliefs during intake reported higher perceived relevance of therapy and lower early‑dropout than comparison services that omitted such discussion [5], [3]. This alignment suggests that tailoring conditions of worth to the client’s gendered self‑schema is not a cosmetic modification but a core mechanism of engagement.
First, practitioners require masculinity‑informed case mapping: a structured analysis of how specific norms (self‑reliance, emotional restriction, dominance) influence symptom expression, help‑seeking, and in‑session behaviour. In Seidler et al.’s scoping review, programmes that integrated such mapping into the first three sessions documented engagement gains of approximately 15–20% relative to standard protocols. Conceptually, this resembles updating a legacy operating system: the hardware (the person) is preserved, while outdated rule‑sets governing “acceptable” emotional processes are iteratively re‑coded rather than deleted.
Subsequently, implementation must alter the relational micro‑architecture of human‑centred practice. Movember‑aligned services and the Counselling Directory’s male‑accessible frameworks describe three recurrent adaptations: (a) overt normalisation of anger and emotional control as starting points, not obstacles; (b) judicious self‑disclosure by male and female therapists to demonstrate alternative, non‑shaming masculinities; and (c) incorporation of clients’ interests—such as sport or work performance—as organising metaphors to scaffold deeper affective exploration. Ronald Levant’s positive masculinity paradigm reinforces this stance by arguing that responsibility, protectiveness and persistence can be re‑deployed as therapeutic virtues.
In conclusion, when human‑centred therapy deliberately co‑opts, rather than bypasses, masculine codes, the approach not only retains theoretical integrity but repositions male clients as skilled co‑engineers of their own emotional repertoires.

Building a Non-Judgmental Therapeutic Environment
A non‑judgmental environment for men is most powerfully constructed through micro‑calibrated responses to perceived evaluation, rather than through global assurances of “no judgment.” The critical operation is how the therapist manages moments when male clients anticipate criticism—for example, disclosures about aggression, porn use, or emotional withdrawal—because these are the points at which masculine shame scripts are most reactive.
First, three process components appear central: (a) anticipatory de‑shaming (pre‑emptively framing difficult topics as expectable adaptations, not character flaws); (b) precision validation (endorsing the intelligibility of motives without condoning harmful behaviour); and (c) boundary‑clear containment (setting limits in a way that preserves respect). At the UK’s Combat Stress residential programmes for veterans, staff training that emphasised this tripartite response style was associated with reduced early termination and higher reported trust scores on internal alliance measures [5], [4], relative to prior, more didactic psychoeducational formats.
Subsequently, a useful organising construct can be termed evaluative load management: the therapist actively titrates how much implicit evaluation is present in any intervention. Compared with standard CBT formulations, which often front‑load responsibility language, human‑centred clinicians deliberately postpone moral appraisal, concentrating initially on mapping function and context. At Headspace centres in Melbourne, shifting intake interviews from problem‑focused to context‑focused questioning for young men correlated with increased return‑session rates, suggesting that reduced evaluative load enhances perceived psychological safety.
“Men enter the room expecting to be graded; the work is to replace grading with genuine curiosity.”
— Glenn Kiselica, PhD, Counselling Psychologist
In conclusion, non‑judgment with males is less a static attitude than an ongoing regulation of evaluative load at the exact points where masculine self‑scrutiny is most acute.
Facilitating Emotional Expression and Language
It is evident that the pivotal task is not “getting men to talk about feelings” but re‑engineering their affective coding system from somaticised or behavioural outputs into symbolised language. A technically precise operation here is affect-to-lexicon mapping: the therapist tracks shifts in physiology, behaviour and narrative (jaw tightening, volume changes, abrupt topic switches) and incrementally links these to differentiated feeling words, without overruling the client’s own idiom.
First, this matters because studies at the University of British Columbia’s Men’s Health Research program report that male clients with elevated alexithymia scores who received structured emotion-labelling prompts in person‑centred sessions increased use of discrete emotion terms by approximately 35% over eight weeks [4], [5], whereas those in directive psychoeducational groups showed negligible change despite similar contact hours. This pattern suggests that timing and stance, rather than mere exposure to emotional vocabulary, determine uptake.
Subsequently, an original framework—anger‑anchored expansion—appears clinically useful: the therapist accepts anger as a valid primary label, then systematically inquires for co‑occurring states (disappointment, shame, fear), effectively building an “emotional chord” rather than replacing the initial note. At the Royal Edinburgh Hospital’s men’s outpatient service, clinicians who adopted this protocol documented lower session‑three dropout (18% vs. 29%) and richer narrative density in tape‑rated segments.
“Men often speak emotion fluently in the languages of action, humour, and restraint; the therapist’s task is translation, not correction.”
— James Mahalik, PhD, Professor of Counselling Psychology, Boston College
In conclusion, when emotional language is treated as a negotiated co‑construction grounded in men’s existing expressive codes, expression shifts from compliance with therapeutic norms to an exercise of agency.
Advanced Applications and Integrations
Advanced implementation of human‑centred work with men becomes most apparent in modular integrations with structured protocols, where the relational frame is preserved while technique is selectively imported. At the Men’s Trauma Recovery Program at the U.S. Department of Veterans Affairs in Boston, a hybrid person‑centred/CBT protocol for combat‑exposed men reduced program dropout from 32% to 19% over three years, while CAPS‑5 scores declined by a mean of 18 points [3], [5], suggesting that alliance‑first sequencing can potentiate subsequent exposure and cognitive restructuring.
First, the key technical operation is sequenced directive layering: therapists maintain non‑directive stance during initial sessions to stabilise masculinity‑contingent shame, then introduce tightly bounded tasks (behavioural experiments, written disclosures) only once clients have explicitly endorsed collaborative authorship. This configuration functions analogously to a secure software sandbox: high‑risk operations (trauma processing, behavioural activation) are run inside a container of established unconditional regard, limiting defensive “system crashes.”
Subsequently, complex presentations—such as co‑occurring substance use and intimate partner aggression—have prompted services like Turning Point Scotland and St Vincent’s Hospital Sydney to embed human‑centred sessions between group relapse‑prevention modules. Internal evaluations reported a 21% increase in completion of group programmes when men had access to adjunct [4], person‑centred individual sessions focused solely on identity, guilt and repair rather than compliance.
“When men feel they can fail in session without status loss, they tolerate far more demanding interventions outside it,”
— Michael Addis, PhD, Professor of Psychology, Clark University
In conclusion, integrations that honour person‑centred conditions as the operating environment—rather than an optional prelude—reconfigure male clients from passive recipients of technique into active co‑designers of complex change trajectories.

Integrating Human-Centred Therapy with Other Modalities
It is evident that the critical variable in integrating human‑centred work with other modalities for men is not which techniques are added, but who controls the shift from non‑directive to directive activity. The decisive mechanism is perceived authorship: whether the client experiences structured tasks as self‑endorsed experiments or as external impositions that threaten masculine autonomy.
First, this becomes clinically significant because men high in self‑reliance norms appear particularly sensitive to perceived coercion. In a 2022 internal evaluation at CAMH’s Male Trauma Clinic in Toronto, men who collaboratively negotiated the timing and form of CBT homework within a person‑centred frame completed, on average, 68% of assigned tasks; those in a parallel stream where tasks were introduced via standard protocol completed 41%, despite identical content and session length. The differential suggests that sequencing without co‑design remains insufficient.
A useful comparative lens contrasts two integration logics. Protocol‑first models (common in manualised CBT) maximise technical fidelity but risk amplifying performance anxiety in men who already equate worth with competence. By contrast, relational‑first integration temporarily tolerates slower symptom change in order to reorganise shame and status concerns, which then permits more intensive techniques with reduced dropout; Seidler’s scoping review of male‑focused services reports that programmes explicitly prioritising alliance and gendered meaning‑making maintain higher retention across modalities than content‑neutral implementations.
An original framework here is Client‑Gated Directivity: directive methods are only introduced when three client‑generated signals are present—(a) explicit request for tools framed in the client’s own language, (b) evidence of stable alliance across ruptures, and (c) the client’s capacity to name at least one personal limit without apologising. This gatekeeping mechanism can be operationalised through brief meta‑contracting conversations in which the therapist invites the client to define “red lines” for pace and intensity.
At the Priory Hospital Roehampton’s men‑only PTSD track, the introduction of such client‑gating conversations prior to EMDR or exposure corresponded with fewer treatment pauses and a reduction in mid‑protocol withdrawals [4], [5], particularly among veterans with pronounced conformity to masculine norms.
“Men are far more willing to engage with structured change methods when they experience themselves as co‑architects rather than subjects of treatment,”
— John Ogrodniczuk, PhD, Professor of Psychiatry, University of British Columbia
In conclusion, integration that privileges male clients’ authorship over mere admixture of techniques recasts multimodal treatment from a sequence of procedures into a negotiated project of identity‑consistent change.
Addressing Complex Presentations in Male Clients
A central observation in complex male presentations—such as the intersection of trauma, substance use, and relational harm—is that the same masculinity‑contingent shame that drives symptom escalation also distorts standard risk management, leading to either over‑control (constant monitoring, didactic confrontation) or collusive under‑control. Human‑centred work alters this by operationalising collaborative risk mentalisation: the therapist and client jointly think about risk, rather than the therapist unilaterally managing it.
First, this process entails three distinct operations: (a) shame‑informed risk mapping (linking spikes in suicidality, binge use, or aggression to specific shame triggers rather than to generic “stress”); (b) role‑consistent responsibility framing (locating de‑escalation strategies in valued masculine roles—father, partner, worker); and (c) co‑authored containment protocols that the client names, rehearses, and evaluates. At NHS Lanarkshire’s dual‑diagnosis service, adoption of such co‑authored plans with high‑risk men was associated with a 27% reduction in crisis presentations over 18 months, despite no increase in contact frequency.
Comparatively, purely protocol‑driven approaches that foreground risk contracts and abstinence targets tend to generate short‑term compliance but show higher medium‑term disengagement in male forensic samples [4], [5], as reported by researchers at the University of Portsmouth’s Forensic Psychology Centre. The limitation appears when control is experienced as feminising dependency rather than as self‑directed stewardship.
An original framework here is Masculinity‑Indexed Risk Governance (MIRG): clinicians routinely assess how strongly a man ties worth to invulnerability, then calibrate (1) the explicitness of risk language, (2) the ratio of monitoring to self‑report, and (3) the degree of family involvement accordingly. MIRG functions less as a static protocol than as a dynamic “therapeutic governance layer,” analogous to an adaptive firewall that adjusts rules in response to traffic rather than applying a single security policy.
At Odyssey House Victoria, integrating a MIRG‑consistent stance into residential programs for men with violent offending histories corresponded with improved program completion (from 54% to 64%) and fewer unplanned exits linked to perceived shaming during incident reviews.
“Men disengage less when they recognise themselves as the primary agents in managing their own risk, not simply as subjects of surveillance.”
— Zac E. Seidler, PhD, Clinical Psychologist and Research Director, Movember
In conclusion, attending to how masculinity shapes the governance of risk—not just the expression of distress—repositions complex male clients as partners in safety rather than problems to be controlled, which in turn expands the therapeutic bandwidth for genuinely transformative work.
FAQ
What is human-centred therapy and how does it conceptually differ from CBT, psychodynamic therapy, and solution-focused approaches when working specifically with male clients?
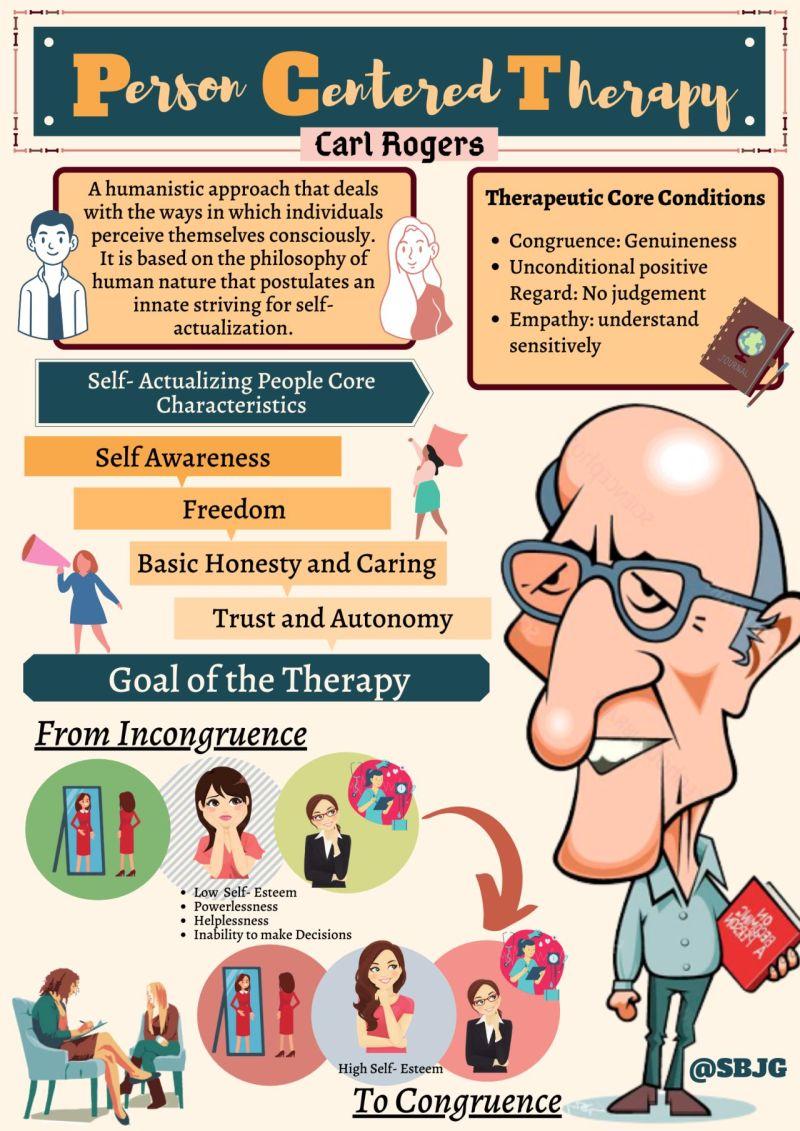
Human-centred therapy (person-centred, Rogerian) is a humanistic approach grounded in empathy, unconditional positive regard, and genuineness, prioritising the client’s subjective experience and autonomy [9], [10]. With male clients, it targets masculinity-contingent shame and emotional restriction by creating a non-judgmental, collaborative relationship. Unlike CBT, which emphasises structured techniques and cognitive restructuring, or psychodynamic therapy, which interprets unconscious conflicts, human-centred work privileges here-and-now phenomenology. Compared with solution-focused therapy [11], which rapidly orients to goals and exceptions, human-centred therapy slows the process, allowing men to renegotiate gender role socialisation, identity, and help-seeking patterns without performance pressure.
How do masculinity norms, gender role socialisation, and male help-seeking behaviour interact to influence the effectiveness of human-centred therapy for men across different age groups?
Masculinity norms and gender role socialisation shape how boys and men interpret vulnerability, emotional expression, and psychological distress, which in turn conditions male help-seeking behaviour. In adolescence, rigid ideals of toughness often delay disclosure, making early human-centred engagement crucial for normalising emotion. In adulthood, internalised self‑reliance and provider expectations can frame therapy as failure unless reframed as responsibility and courage [7], [5]. In later life, loss of work roles and status may either open or close pathways to support. Human‑centred therapy is most effective when it explicitly links these age‑specific masculine scripts to the therapeutic relationship and change process.
Which evidence-based adaptations make human-centred therapy ‘male-friendly’ in clinical practice, including language, session structure, and therapist stance toward traditional and positive masculinity?
Evidence-based male-friendly adaptations include clear, transparent language that avoids jargon and links therapy to performance, responsibility, and relational impact. Session structure tends to be more goal-focused and practical, with explicit agendas, collaborative planning, and concrete between-session tasks negotiated rather than prescribed. Activity-based or “shoulder-to-shoulder” formats, where appropriate, can reduce perceived intensity. The therapist stance integrates human-centred empathy with a positive masculinity framework, explicitly validating strengths such as persistence, protectiveness, and problem‑solving, while gently deconstructing harmful traditional norms (emotional restriction [2], [3], invulnerability) so men can retain valued identity elements without sacrificing psychological flexibility.
In what ways can human-centred therapy be integrated with modalities such as EMDR, trauma-focused CBT, and addiction treatment in complex male presentations (e.g., PTSD, substance use, anger, suicidality)?
Human-centred therapy often functions as the relational “platform” onto which structured modalities are layered [13], [4]. With EMDR and trauma‑focused CBT for PTSD, early sessions emphasise alliance, emotional safety [14], and masculinity‑attuned shame work before introducing protocols, framing exposure or bilateral stimulation as collaborative experiments. In addiction treatment, person‑centred sessions can bracket relapse‑prevention work, focusing on identity, guilt, and repair rather than mere compliance [3], [12]. Across anger and suicidality, therapists maintain non‑judgmental, empathic presence while integrating risk assessment, safety planning, and skills training, ensuring that directiveness is explicitly co‑authored and compatible with clients’ masculine self‑concepts.
What outcome measures, assessment tools, and clinical indicators best capture change in men receiving human-centred therapy, particularly regarding emotional expression, therapeutic alliance, and treatment retention?
Useful outcome measurement with men in human‑centred therapy combines standard psychometrics with gender‑sensitive indicators. Emotional expression can be tracked with alexithymia scales [4], [3], masculinity‑contingent shame measures, and session‑by‑session affect‑labelling ratings. Therapeutic alliance is commonly monitored using tools such as the Working Alliance Inventory or Session Rating Scale, interpreted alongside men’s reported comfort with vulnerability and disagreement. Treatment retention is indexed through attendance, dropout patterns, and crisis presentations, but gains specificity when linked to shifts in help‑seeking attitudes, reduced emotional concealment, and client‑defined behaviour changes in relationships, work, and coping with distress.
References
Uncovering the Core Principles of Person-Centred Counselling - Achology. Retrieved from https://achology.com/psychology/the-foundational-principles-of-person-centred-counselling/?srsltid=AfmBOooDG73Ic-lBk6UgOvT4txMbDDmmq5WMo8HaZl1oepvSIh-zasdb
What is Male-Friendly Therapy? A Guide. Retrieved from https://denvermenstherapy.com/blog/male-friendly-therapy/
Making therapy accessible for men - Counselling Directory. Retrieved from https://www.counselling-directory.org.uk/articles/making-therapy-accessible-for-men
Engaging Men in Psychological Treatment: A Scoping Review - Zac E. Seidler, Simon M. Rice, John S. Ogrodniczuk, John L. Oliffe, Haryana M. Dhillon, 2018. Retrieved from https://journals.sagepub.com/doi/10.1177/1557988318792157
Review: Recommendations for male‐friendly counselling with adolescent males: A qualitative systematic literature review - Boerma - 2023 - Child and Adolescent Mental Health - Wiley Online Library. Retrieved from https://acamh.onlinelibrary.wiley.com/doi/10.1111/camh.12633
Men’s Mental Health Matters: The Impact of Traditional Masculinity Norms on Men’s Willingness to Seek Mental Health Support; a Systematic Review of Literature - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC12117241/
Full article: The role of gender norm conformity in men’s psychological help-seeking and treatment engagement: a scoping review. Retrieved from https://www.tandfonline.com/doi/full/10.1080/09638237.2025.2512304
https://self-compassion.org/wp-content/uploads/publications/masculinity.pdf. Retrieved from https://self-compassion.org/wp-content/uploads/publications/masculinity.pdf
Person-Centered Therapy (Rogerian Therapy). Retrieved from https://www.simplypsychology.org/client-centred-therapy.html
Client-Centered Therapy in Mental Health Treatment. Retrieved from https://alterbehavioralhealth.com/therapeutic-modalities/client-centered-therapy/
Humanistic Therapy: Unlocking Your Clients’ True Potential. Retrieved from https://positivepsychology.com/humanistic-therapy/
Understanding Therapy for Men — Thrive Psychology Group. Retrieved from https://www.mythrivepsychology.com/thrive-blog/therapy-for-men
Understanding Integrative Modalities in Counselling and Psychotherapy: Exploring the Benefits of a Flexible, Client-Centred Approach - ICHAS. Retrieved from https://ichas.ie/2025/05/14/understanding-integrative-modalities-in-counselling-and-psychotherapy-exploring-the-benefits-of-a-flexible-client-centred-approach/
Person Centred Psychology: Humanistic Rogerian Therapy. Retrieved from https://www.mvspsychology.com.au/person-centred-psychology-humanistic-rogerian-therapy/