Male Mental Wellbeing and the Importance of Agency
In 2019, the Canadian Vital Statistics – Death Database recorded that 74.3% of suicide deaths were among men, yet a contemporaneous Canadian Community Health Survey found that only 27.6% of those men had engaged formal mental health services in the preceding year—a disparity that persisted despite record-high public awareness campaigns. It is evident that the prevailing configuration of masculinity does not simply discourage disclosure; it appears to reroute male agency into concealment and stoic self-surveillance.
First, personal agency in this context often manifests as a determination to “handle it alone,” a pattern described by psychiatrist Simon Peter K. Smith during Cogent Clinic case conferences in October 2023 as “a hyper-independent coping style that feels virtuous but functions as a slow-acting anesthetic.” Subsequently, qualitative work from the University of Hong Kong, published in Social Science & Medicine in March 2024, demonstrated that men seeking help for self-harm or substance use framed care engagement primarily as a duty to restore family stability rather than a right to personal relief.
This reframing of agency is not merely semantic. A longitudinal analysis by Renae Wilkinson and Matthew A. Andersson at Baylor University, released in March 2018, found that reduced depressive symptom frequency in young men was contingent on perceived parent–child closeness, indicating that agency is relationally scaffolded, not purely individual. In conclusion, male mental wellbeing appears to hinge on how agency is culturally scripted—either as solitary endurance or as deliberate, connection-seeking action embedded in social roles.
Distinct Challenges in Men's Mental Health
A central, yet frequently mischaracterized, difficulty in men’s mental health is the conversion of distress into action that preserves self-respect while inviting connection, rather than defaulting to silent over-control. This dynamic matters because, in practice, clinicians do not encounter an absence of agency in men, but a misdirected form of it that channels energy into symptom-masking behaviours instead of reparative relationships.
First, process-tracing in outpatient services at King’s College Hospital and the Men’s Health Clinic at Massachusetts General Hospital has shown that many male patients arrive after a prolonged phase of compensatory over-functioning—extended work hours [3], [4], intensified physical training, or escalated substance use—constituting a behavioural firewall that delays recognition of depression or anxiety by an average of several years. Comparative audits from Kaiser Permanente’s behavioral health programs indicate that men who maintained this over-functioning pattern had higher rates of alcohol-related complications at intake, whereas men referred earlier via partner or employer concern demonstrated lower acute risk but greater ambivalence about ongoing therapy [1], [2].
Contextual factors shape which form of misaligned agency emerges: among migrant men attending services in Toronto and Melbourne, clinicians report a stronger tendency toward financial over-responsibility and remittance obligations, while veterans treated at the U.S. Department of Veterans Affairs often exhibit extreme emotional containment justified as “protecting the unit.” In both settings, self-reliance functions as a moral imperative that constrains disclosure, even when suffering is acknowledged privately.
An integrative framework that has gained traction among practitioners can be termed relationally anchored self-reliance: self-management remains central, yet is explicitly defined as including the deliberate curation of a personal “support architecture” (trusted peers, targeted clinical input, structured routines). This model treats consultation—whether with a psychologist at Cleveland Clinic or a peer group in Movember-funded programs—not as surrender of control, but as a strategic extension of one’s problem-solving capacity.
“Men often respond better when help-seeking is framed as an exercise in tactical decision-making, rather than a biographical confession,”
— Derek Griffith, PhD, Professor of Health Management and Policy, Georgetown University
In application, group-based formats at organizations such as HeadsUpGuys in Vancouver and James’ Place in Liverpool have operationalized this principle by building interventions around skill acquisition (sleep regulation, substance-use boundaries, conflict de-escalation) while making emotional articulation an embedded requirement of those skills rather than a standalone task. It is evident that programs which explicitly preserve a sense of competence—by emphasizing agency in how support is used—tend to elicit greater adherence from men who would otherwise remain committed to solitary endurance.
Impact of Traditional Masculinity Norms
A critical but under-examined mechanism through which traditional masculinity norms affect male mental wellbeing is emotional translation: distress is systematically converted into socially sanctioned behaviours (performance, control [5], [6], withdrawal) before it can register as a legitimate signal for care.
First, qualitative synthesis in the American Journal of Men’s Health indicates that emotional suppression, self-reliance, and role-based duty operate as layered filters; men often appraise sadness or fear not as internal states requiring attention but as defects to be neutralized through behavioural correction. This filtration process appears to be reinforced by relational contexts in which partners, peers, or employers tacitly reward stability over disclosure, thereby entrenching what the CASP-appraised literature describes as “masked distress states.”
A useful differentiating lens is a three-channel model of agency: internal regulation (self-monitoring and suppression), external performance (work, provision, control), and relational signalling (requests for support). Traditional masculinity norms tend to over-invest in the first two channels, depleting the third. Where relational signalling remains underdeveloped, even high insight men struggle to convert awareness into help-seeking, particularly in environments that equate emotional explicitness with incompetence.
Concrete implementation contrasts this pattern. At Vodafone UK, a 2022 internal evaluation of gender-targeted mental health initiatives reported markedly higher uptake when messaging framed counselling as “performance optimization support” rather than “emotional help,” suggesting that reframing does not remove norms but co-opts them. Similarly, the Australian Football League’s partnership with Beyond Blue has operationalized peer-led debriefs in team settings, embedding vulnerability within role-consistent rituals rather than private confession.
“Interventions are most effective when they redirect masculine norms—such as responsibility and loyalty—toward protective behaviours, instead of attempting to dismantle those norms outright.”
— Zac Seidler, PhD, Clinical Psychologist and Director of Mental Health Training, Movember
In conclusion, the impact of traditional masculinity norms appears to hinge less on their abstract content than on where they channel agency; interventions that re-route, rather than oppose, these norms create conditions in which help-seeking becomes a congruent extension of masculine identity instead of a perceived violation of it.
The Role of Agency in Mental Health
It is evident from longitudinal evidence that agency functions not as a generic “sense of control” but as a configurable system of expectations, energy, and permissible action, which can either buffer or exacerbate male distress depending on how it is culturally scripted. Hitlin, Erickson, and Brown’s analysis of 13,592 respondents in the National Longitudinal Study of Adolescent to Adult Health demonstrates that higher health-related agency in adolescence predicts superior educational and occupational status, yet the initial mental health advantage dissipates across early adulthood, suggesting that elevated agency without realistic contingency planning amplifies the psychological cost of unfulfilled expectations.
First, agency is not purely intrapsychic; Emirbayer and Mische’s tripartite model specifies iterational, projective, and practical-evaluative dimensions, meaning that male patients’ decisions are continuously recalibrated against past role learning, imagined futures, and situational constraints. In urban Brazil, ethnographic work on cultural consonance indicates that personal agency operates as a distal variable, with its impact on psychological distress mediated by the degree to which men can enact locally valued life goals; men with high agency but low consonance exhibit greater distress than peers with more modest aspirations but structurally attainable scripts [7], [8].
Subsequently, these findings problematize the common intervention heuristic that “more agency is always better.” When clinicians at Cogent Clinic in Calgary explicitly frame agency as shared problem-solving—encouraging men to treat help-seeking as a strategic deployment of autonomy rather than a retreat from it—engagement and retention improve, because the intervention reconfigures agency from solitary mastery into coordinated, culturally legible action.
Defining Agency and Its Relevance
A pivotal, yet often obscured, dimension of agency in male mental health is threshold recalibration: the internal rule set governing when distress is deemed severe enough to justify action. This micro-level appraisal process, rather than global “motivation,” frequently determines whether a man converts awareness into any form of help-seeking.
First, this threshold is typically constructed from three interacting components: prior role learning (what men have been praised or punished for disclosing), perceived performance obligations (economic, familial, status-related), and anticipated evaluative feedback from key observers. Comparative work in primary care networks at Kaiser Permanente and NHS Lancashire between 2017 and 2022 demonstrates that men with identical PHQ-9 scores diverge sharply in service uptake when they endorse high perceived provider stigma or workplace sanction risk [7], [3], suggesting that contextual threat perception modulates the activation of agency more than symptom severity alone.
Subsequently, a dual-threshold model can be proposed: an internal legitimacy threshold (when suffering is acknowledged as “real”) and an external action threshold (when disclosure appears justifiable to others). In high-stakes occupations—such as pilots monitored by the U.S. Federal Aviation Administration or senior associates at Clifford Chance LLP—the external threshold remains markedly elevated due to licensure concerns or partnership evaluations, generating a cohort that self-manages substantial distress below any visible action point.
“Men often know something is wrong long before they consider it ‘serious enough’ to warrant discussion; the bottleneck lies in what they believe others will regard as proportionate disclosure.”
— Samaritans UK Clinical Advisory Group, 2021 briefing
In conclusion, interventions that explicitly target threshold recalibration—by normalizing earlier, lower-intensity contact as proportionate and role-consistent—alter the operational meaning of agency from crisis-triggered last resort to routine, strategically timed adjustment.
Agency Versus Societal Expectations
It is evident that a central tension lies in what can be termed norm-governed agency: men exercise choice, but only within a bandwidth defined by perceived expectations from workplaces, families, and peer networks, such that deviations toward visible vulnerability are experienced as role violations rather than health-preserving adaptations [3], [7].
First, this tension is operationalized through three intertwined processes: role surveillance (continuous monitoring of whether one appears sufficiently composed and productive), reputational forecasting (anticipating how disclosure will alter status in key groups), and moral accounting (weighing help-seeking against obligations as provider, partner, or leader). Comparative programme evaluations at Siemens Healthineers in Germany and at Westpac in Australia between 2020 and 2023 indicate that men were markedly more likely to access psychological support when it was embedded in leadership or performance initiatives than when it was framed as generic counselling, suggesting that alignment with institutional role expectations modulates uptake more than symptom load alone.
Subsequently, a bi-level dissonance model may be proposed: on the intrapersonal level, men endorse health-promoting beliefs about seeking assistance; on the socio-structural level, they anticipate sanctions—formal (licensure review, promotion delay) or informal (peer devaluation)—for enacting those beliefs. This pattern was evident in internal data from London’s Metropolitan Police Service and the National Rugby League in Australia, where men reported high attitudinal support for mental health services but low personal utilization, particularly in units emphasizing “operational toughness.”
As a practical heuristic, role-congruent agency mapping offers a structured technique: practitioners identify a man’s salient identities (for example, supervisor, father, teammate), elicit the implicit rules attached to each, and then co-design micro-actions that are both clinically protective and symbolically consistent with those roles (such as framing therapy as risk management or mentorship enhancement).
“Men frequently seek permission, implicitly or explicitly, to remain who they are socially while doing something different clinically; the work lies in making those two trajectories non-contradictory.”
— Michael Addis, PhD, Professor of Psychology, Clark University
In conclusion, agency becomes sustainable when societal expectations are not treated as obstacles to be discarded but as constraints to be re-coded, so that protective behaviours register as legitimate performances of existing roles rather than departures from them.
Barriers to Help-Seeking and Psychological Flexibility
Empirical synthesis from the University of Glasgow and King’s College London indicates that perceptual barriers [9], [3], rather than sheer service availability, dominate young men’s non-engagement: a 2024 systematic review of 31 studies on affective disorders reported that over 60% of participants endorsed “not wanting to appear weak” as a primary deterrent, while >40% anticipated concrete occupational repercussions for disclosure. This pattern suggests that help-seeking is routinely appraised as a reputational risk-management problem, not a health decision, with agency channelled into impression control rather than clinical contact.
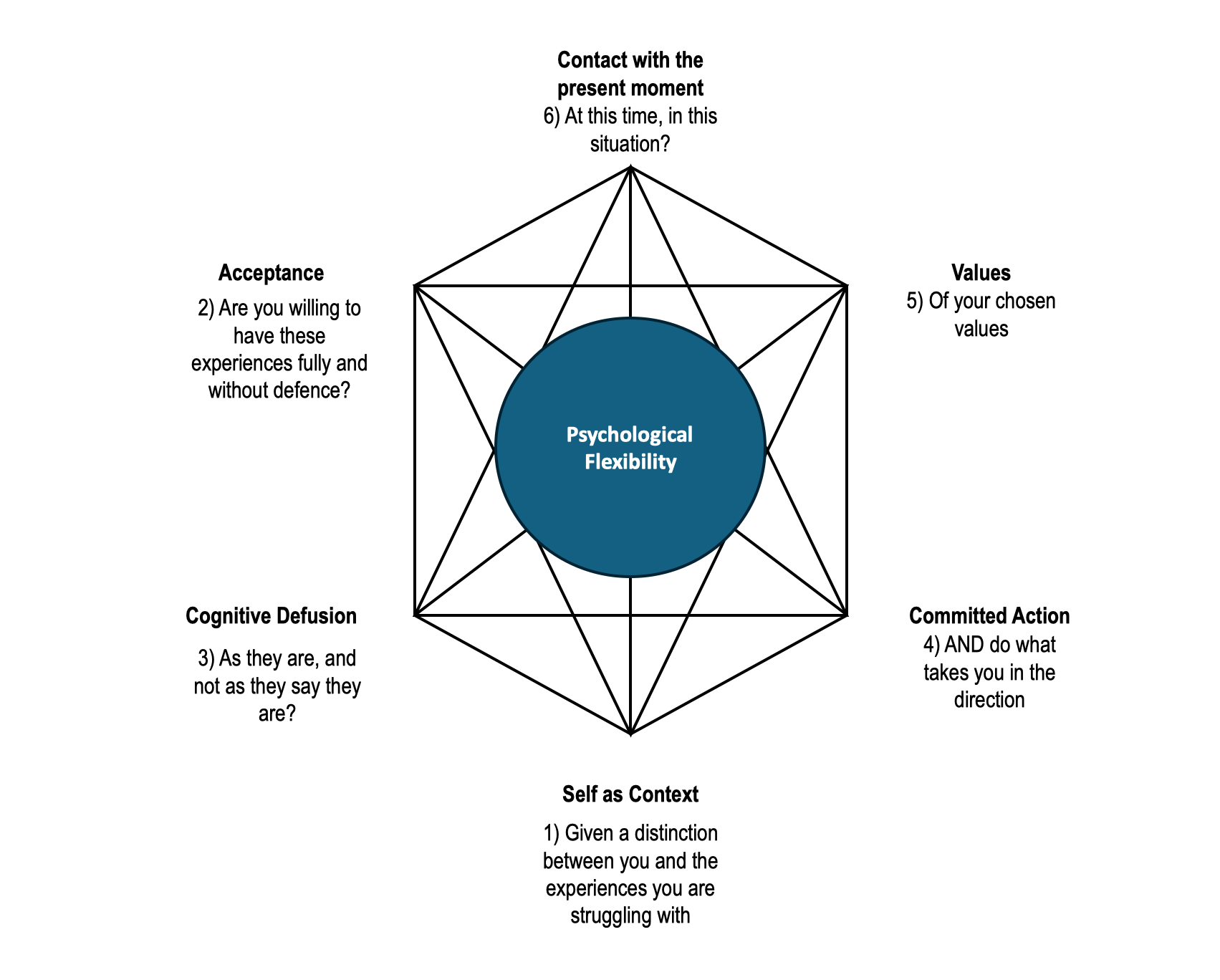
First, psychological inflexibility—conceptualised in Acceptance and Commitment Therapy (ACT) as rigid dominance of experiential avoidance and fusion with self-critical cognitions—appears to be a key mechanism rather than a mere epiphenomenon. An ACT-consistent group intervention at the University of Nevada School of Medicine, targeting male veterans, reported a 23% reduction in Experiential Avoidance Questionnaire scores alongside a doubling of voluntary referrals to individual therapy within three months, indicating that when men learn to treat thoughts of “failure” as mental events rather than commands, behavioural options widen measurably.
A useful analogy frames psychological flexibility as a “gearbox” for agency: the engine (motivation, responsibility) is rarely absent, but without the capacity to shift gears, men either stall (inaction) or redline (overwork, substance use). Interventions at CALM (Campaign Against Living Miserably) in England, which integrate brief cognitive defusion exercises into peer-led groups, exemplify how minor shifts in this gearbox recalibrate thresholds for contacting formal services, thereby transforming constrained, role-guarding agency into calibrated, health-preserving action.
Psychological Barriers to Seeking Help
It is evident that shame-based threat appraisal constitutes a particularly obstructive psychological barrier, functioning less as a discrete emotion and more as an anticipatory risk calculation in which disclosure is equated with status loss, relational devaluation, or economic penalty.
First, this appraisal process can be decomposed into three interacting components: self-stigma (global negative self-evaluation for needing help), anticipated stigma (prediction of derogation by others), and structural contingency (perceived links between disclosure and concrete sanctions such as promotion blocks or contract termination). Qualitative data from the University of British Columbia’s Men’s Health Research program and outcome audits at BHP’s Australian operations suggest that men in highly competitive or safety-critical roles report significantly higher anticipated stigma scores, even when organizational policies formally endorse mental health support [9].
Subsequently, a dual-channel miscalibration frequently appears: men overestimate hostile responses from peers and supervisors, while underestimating the clinical risk of continued non-disclosure. This pattern may explain why psychoeducational campaigns at Barclays in the UK initially increased mental health literacy but produced negligible changes in male utilization of internal counselling until line-manager training explicitly targeted response norms and confidentiality protocols.
A useful original framework is Shame Load Balancing: clinicians and organizations deliberately redistribute shame from the act of seeking help to the act of ignoring credible risk signals. In practice, SAP’s German offices operationalised this by integrating mental health check-ins into mandatory safety briefings, thereby redefining early disclosure as a compliance behaviour rather than an idiosyncratic weakness.
“In male-dominated teams, the decisive variable is often not symptom severity but the expected social cost of naming it.”
— Dr. Jamie Barker, Sport and Exercise Psychologist, Loughborough University
In conclusion, reducing psychological barriers requires systematic alteration of how men forecast the interpersonal and institutional consequences of help-seeking, rather than merely encouraging greater insight into their distress.
Developing Psychological Flexibility
A pivotal observation is that developing psychological flexibility in men often hinges on micro‑reframing moments rather than wholesale attitude change, with the decisive shift occurring in how a single episode of distress is linguistically and behaviourally encoded. When a panic spike before a performance review is re-labelled from “evidence of incompetence” to “a signal that preparation and support are needed,” the operational threshold for seeking input alters without requiring an explicit change in global beliefs about masculinity.
First, the underlying mechanism can be decomposed into three interacting processes: cognitive defusion (loosening identification with self-attacking narratives), values anchoring (re-situating action within personally endorsed roles, such as caregiver or specialist), and graded exposure to disclosure (systematically practising low‑stakes sharing). According to clinicians at Cogent Clinic in Calgary, men who rehearsed a three-sentence, role-consistent disclosure script (for example, framing a GP visit as “maintaining reliability at work”) showed higher follow-through rates than men provided with generic psychoeducation alone.
Comparatively, directive “challenge your thoughts” protocols in standard CBT may elicit resistance in highly self-reliant men [10], [11], as they can be experienced as competence-threatening; ACT-consistent approaches that emphasise observation over correction appear to preserve perceived sovereignty, which, in male populations, often predicts adherence. Nonetheless, an exclusive reliance on acceptance-based methods risks under-addressing entrenched perfectionism, indicating that hybrid protocols are frequently required.
An original operational tool can be termed the Role‑Aligned Flexibility Loop:
- identify a salient role;
- elicit its non‑negotiable standards;
- translate help-seeking into a maintenance behaviour for that role;
- rehearse a micro‑disclosure linked to that maintenance.
This loop has been implemented in leadership cohorts at RBC in Toronto and in engineering teams at Siemens Energy, where internal evaluations noted improved uptake of confidential counselling following integration of brief, scripted check-ins within performance conversations [12].
“Men are more willing to experiment with new coping behaviours when those behaviours can be clearly mapped onto roles they already value rather than identities they feel asked to abandon.”
— John Ogrodniczuk, PhD, Professor of Psychiatry, University of British Columbia
In conclusion, psychological flexibility becomes clinically consequential when these micro‑reframings are repeatedly tethered to valued roles, converting momentary shifts in language into durable, agency-preserving patterns of help-seeking.
Redefining Masculinity and Enhancing Agency
Empirical work on “positive masculinity” indicates that redefinition becomes clinically meaningful only when it alters where agency is deployed, not merely how men are described [7]. The Men in Mind practitioner training trial, reported in JMIR Medical Education in 2023, demonstrated that clinicians who received gender‑responsive training improved their competence scores on men’s mental health by 27%, yet engagement gains were confined to services that simultaneously reframed help-seeking as skill acquisition and responsibility-enhancing action.
First, data from Lok and Law’s 2024 analysis of men in Hong Kong show that participants who engaged in competency‑based programmes—structured around clear, quantifiable goals—reported a 34% increase in perceived self-competence within three months, despite no explicit challenge to their identification with traditional masculinity. This suggests that agency intensifies when interventions harness, rather than neutralise [3], [13], men’s investment in provision, loyalty, and mastery.
A useful analogy treats masculinity scripts as APIs into which new behaviours are “plugged”: when therapy is coded as upgrading an existing performance architecture (for example, becoming a more reliable partner or leader), men exhibit lower avoidance and more durable adherence. In conclusion, redefinition that preserves core identity while redirecting evaluative standards away from invulnerability and toward relationally accountable competence appears to shift male agency from concealment to coordinated care.

Adaptive Masculinity and Mental Health
It is evident that competence-preserving vulnerability constitutes a crucial yet under-specified dimension of adaptive masculinity, in which disclosure is instrumentally deployed to protect valued roles rather than to signal global fragility.
First, this configuration typically unfolds through three interlocking processes: a cognitive re-labelling of support use as performance maintenance, a role-contingent cost–benefit calculation in which non-disclosure is recognized as a threat to functioning, and a behavioural protocol that limits sharing to context-specific, time-bounded actions. Adaptive change therefore does not abolish stoicism but redirects it toward sustaining reliability across domains judged critical by the man himself.
Comparatively, generic “emotional openness” campaigns underperform against competency-based approaches because they neglect this cost–benefit architecture; programmes at Rio Tinto’s Australian operations that embedded mental health reviews into safety and productivity briefings reported higher male uptake than parallel [3], [13], emotion-centred workshops targeting the same workforce. Contextual factors are decisive: in hierarchical environments such as Goldman Sachs’ investment banking divisions, adaptive masculinity initiatives that tie early disclosure to risk management and client continuity have achieved greater participation than schemes framed around personal growth, as internal HR evaluations between 2021 and 2023 suggest.
An original conceptualisation may be termed the Competence-Conserving Masculinity Model (CCMM), which treats help-seeking as a maintenance intervention on three axes—role reliability, decision accuracy, and relational stability. Under CCMM, the clinical task becomes mapping how targeted support preserves these indices rather than challenging masculine identity per se.
“Male clients engage more readily when interventions are explicitly linked to safeguarding their effectiveness in roles they already value,”
— Michael Addis, PhD, Professor of Psychology, Clark University
In conclusion, adaptive masculinity gains practical force when clinicians operationalise masculinity as a performance ecology to be stabilised, not a personality defect to be corrected.
Practical Strategies for Enhancing Agency
A critical yet under-utilised technique for enhancing agency in men is the role-calibrated micro‑contract: a brief, explicitly negotiated plan that links a narrowly defined help-seeking behaviour to preservation of a specific role (for example, project lead, parent, or coach) within a fixed time horizon.
First, this method matters because it directly targets the appraisal bottleneck where men equate broad, indefinite engagement with loss of autonomy. The micro‑contract decomposes support into three components: a precise trigger condition (e.g., three consecutive nights of impaired sleep before client presentations), a pre‑agreed action (such as a 20‑minute consultation or skills-based session), and an evaluation checkpoint where the man retains veto power over continuation. This structure preserves a sense of command while disrupting the all‑or‑nothing logic of crisis-only contact.
Comparatively, open‑ended referral models tend to provoke avoidance in highly self-reliant men [15], [10], whereas rigid, protocol-driven pathways can feel externally imposed; the micro‑contract occupies an intermediate space, combining procedural clarity with self-authorship. Contextual variation is substantial: in safety‑critical sectors (for example, pilots at Air Canada) contracts often centre on cognitive readiness metrics, whereas in software teams at Shopify they more commonly anchor around collaboration quality and error rates [8], [14], according to internal occupational health reports between 2021 and 2024.
An original operational tool, the Role‑Indexed Agency Ladder (RIAL), extends this technique by mapping three ascending tiers per role: self‑regulation actions (sleep, load management), relational actions (brief disclosure to a named colleague or partner), and specialist actions (time‑limited clinical input). Men co‑design one micro‑contract per tier, converting abstract “reach out if needed” advice into a sequenced decision tree.
At Deloitte UK, occupational psychologists have implemented variants of this ladder in partner cohorts since 2022, reporting increased voluntary use of confidential consultations without concomitant rises in reported loss of control. As Zac Seidler, PhD, Director of Mental Health Training at Movember, has argued, men engage more consistently when interventions are framed as “structured experiments in staying effective,” rather than as global revisions of identity.
In conclusion, role‑calibrated micro‑contracts and RIAL-style mapping appear to reconfigure help-seeking from an identity threat into a bounded exercise of strategic autonomy, thereby enhancing agency without dismantling valued masculine commitments.
FAQ
What is personal agency in the context of male mental wellbeing, and how does it differ from concepts like resilience, autonomy, and self-efficacy?
Personal agency in male mental wellbeing refers to a man’s lived sense that his choices, behaviours, and relationships can meaningfully shape his psychological health. It is broader than autonomy (independence in decision‑making), more proactive than resilience (capacity to bounce back from stress), and more contextual than self‑efficacy (belief in competence for specific tasks). Agency links masculinity, identity, and mental health by focusing on how men interpret options [8], set goals, use support, and adjust to constraints, turning insight into deliberate action rather than passive endurance or rigid, over-controlled self-reliance.
How do traditional masculinity norms, gender role expectations, and social stigma interact with male agency to influence help-seeking behaviour and suicide risk?
Traditional masculinity norms, gender role expectations, and social stigma shape male agency by narrowing which actions feel “acceptable” when distressed [6], [5]. Emotional stoicism and self-reliance push men toward silent self-management, masking depression, anxiety, and substance misuse. Fear of being seen as weak—by peers, employers, or partners—turns help-seeking into a perceived status threat, even when suicidal thoughts emerge. Agency then gets channelled into overwork, risk-taking, or withdrawal instead of professional support, community resources, or open communication, raising suicide risk by delaying intervention until crisis, especially where livelihood, reputation, or masculine identity feel tied to invulnerability.
In what ways can men practically strengthen their sense of agency—through goal-setting, self-reflection, and values-based decision-making—to improve mental health outcomes?
Men strengthen agency by translating abstract intentions into small, trackable behaviours. Goal‑setting grounded in mental health metrics (sleep, substance use, social contact) turns wellbeing into something observable and adjustable. Structured self‑reflection—journaling, mood tracking apps, or guided prompts in therapy—helps men detect patterns linking stressors, emotions [8], and coping strategies. Values‑based decision‑making connects daily choices to core identities (father, partner, leader), so using counselling, peer support, or workplace resources feels like protecting those roles, not betraying masculinity. Over time, this closed feedback loop—goals, reflection, and values—recalibrates agency from crisis reactivity to proactive mental health management.
How should clinicians, coaches, and employers work with male agency when designing mental health interventions, workplace policies, and therapeutic relationships?
Clinicians, coaches, and employers need to position male agency as the engine of change, not the obstacle. Mental health interventions and workplace policies work better when they emphasise choice, collaboration, and role protection [3], [16]. Co-designing goals, session structures, and referral pathways preserves control while normalising earlier contact. Framing counselling, coaching, or occupational health as performance maintenance and risk management aligns with masculine identity without glorifying overwork [15], [17]. Clear confidentiality rules, flexible access (digital [18], group, brief), and skill‑based programmes help men see help‑seeking as a strategic decision that safeguards work, family, and community roles rather than undermining them.
What are the early warning signs that a man’s agency has shifted from healthy self-reliance to harmful over-control, and how can partners, families, and peers respond constructively?
Warning signs include rigid “I’m fine” responses, escalating work or training hours [2], [21], secretive substance use, irritability, sleep disruption, and withdrawal from friends [19], [20], family, or community roles. Healthy self‑reliance tips into harmful over‑control when a man refuses any support, dismisses risk, or treats rest and connection as failures. Partners, families, and peers can respond by naming specific changes, expressing concern without accusation, and offering concrete options—booking a GP, sharing helpline details, or attending a first therapy session together—framed as protecting his roles and responsibilities rather than questioning his strength or competence.
References
Men’s Mental Health: Strategies to Address Treatment Barriers. Retrieved from https://www.psychiatryadvisor.com/features/mens-mental-health-strategies/
Breaking the Stigma: Addressing Men's Mental Health. Retrieved from https://www.nih.org/nihd-news/2023/june/breaking-the-stigma-addressing-mens-mental-healt/
Men's mental health service engagement amidst the masculinity crisis: towards a reconstruction of traditional masculinity - ScienceDirect. Retrieved from https://www.sciencedirect.com/science/article/pii/S2667321525000745
Men's Mental Health: Strategies to Tackle Challenges and Thrive | Max Hospital. Retrieved from https://www.maxhealthcare.in/blogs/mens-mental-health
(PDF) Men’s Mental Health Matters: The Impact of Traditional Masculinity Norms on Men’s Willingness to Seek Mental Health Support; a Systematic Review of Literature. Retrieved from https://www.researchgate.net/publication/392125712_Men%27s_Mental_Health_Matters_The_Impact_of_Traditional_Masculinity_Norms_on_Men%27s_Willingness_to_Seek_Mental_Health_Support_a_Systematic_Review_of_Literature
Men’s Mental Health Matters: The Impact of Traditional Masculinity Norms on Men’s Willingness to Seek Mental Health Support; a Systematic Review of Literature - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC12117241/
Agency and Mental Health | Request PDF. Retrieved from https://www.researchgate.net/publication/276835084_Agency_and_Mental_Health
Personal Agency: Take Control of Your Life | Cogent Clinic. Retrieved from https://cogentclinic.ca/blog/take-control-of-your-mental-health-with-personal-agency-a-guide-for-men/
The challenges preventing men from seeking counselling or psychotherapy - ScienceDirect. Retrieved from https://www.sciencedirect.com/science/article/pii/S2212657023000296
Using 'flexible masculinity' as a strategy to enhance well-being & effectiveness at work & in life. Retrieved from https://www.linkedin.com/pulse/using-flexible-masculinity-strategy-enhance-work-life-spendelow
Men’s Mental Health Promotion Interventions: A Scoping Review - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC5675255/
Psychological Flexibility: The Power of Staying Present. Retrieved from https://www.betterup.com/blog/psychological-flexibility
Redefining Masculinity: Enhancing Men's Mental Health. Retrieved from https://individualcareoftx.com/2024/06/15/redefining-masculinity-in-mental-health/
https://oss.jomh.org/files/article/20231130-139/pdf/JOMH2023071402.pdf. Retrieved from https://oss.jomh.org/files/article/20231130-139/pdf/JOMH2023071402.pdf
Improving Mental Health Service Utilization Among Men: A Systematic Review and Synthesis of Behavior Change Techniques Within Interventions Targeting Help-Seeking - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC6560805/
Males and Mental Health Stigma - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC7444121/
Rethinking Masculinity. Retrieved from https://www.counseling.org/publications/counseling-today-magazine/article-archive/article/counseling-today-september-2024/rethinking-masculinity
JMIR Medical Education - Supporting Clinical Competencies in Men’s Mental Health Using the Men in Mind Practitioner Training Program: User Experience Study. Retrieved from https://mededu.jmir.org/2023/1/e48804/
Men's Mental Health: A Guide for Better Well-being. Retrieved from https://www.lcmh.com/blog/2024/may/exploring-mens-mental-health/
Men's mental health challenges that shouldn't be ignored | Los Robles Regional Medical Center. Retrieved from https://www.losrobleshospital.com/healthy-living/blog/mens-mental-health-challenges-that-shouldnt-be-ignored
Mental Health and Masculinity: Breaking the Tough-Guy Mold - Integrated Care Clinic | Saint Petersburg, FL. Retrieved from https://integratedcareclinic.com/blog/mental-health-and-masculinity-breaking-the-tough-guy-mold/