Prevalence and Causes of PTSD in Male Military Veterans vs. Civilian Men
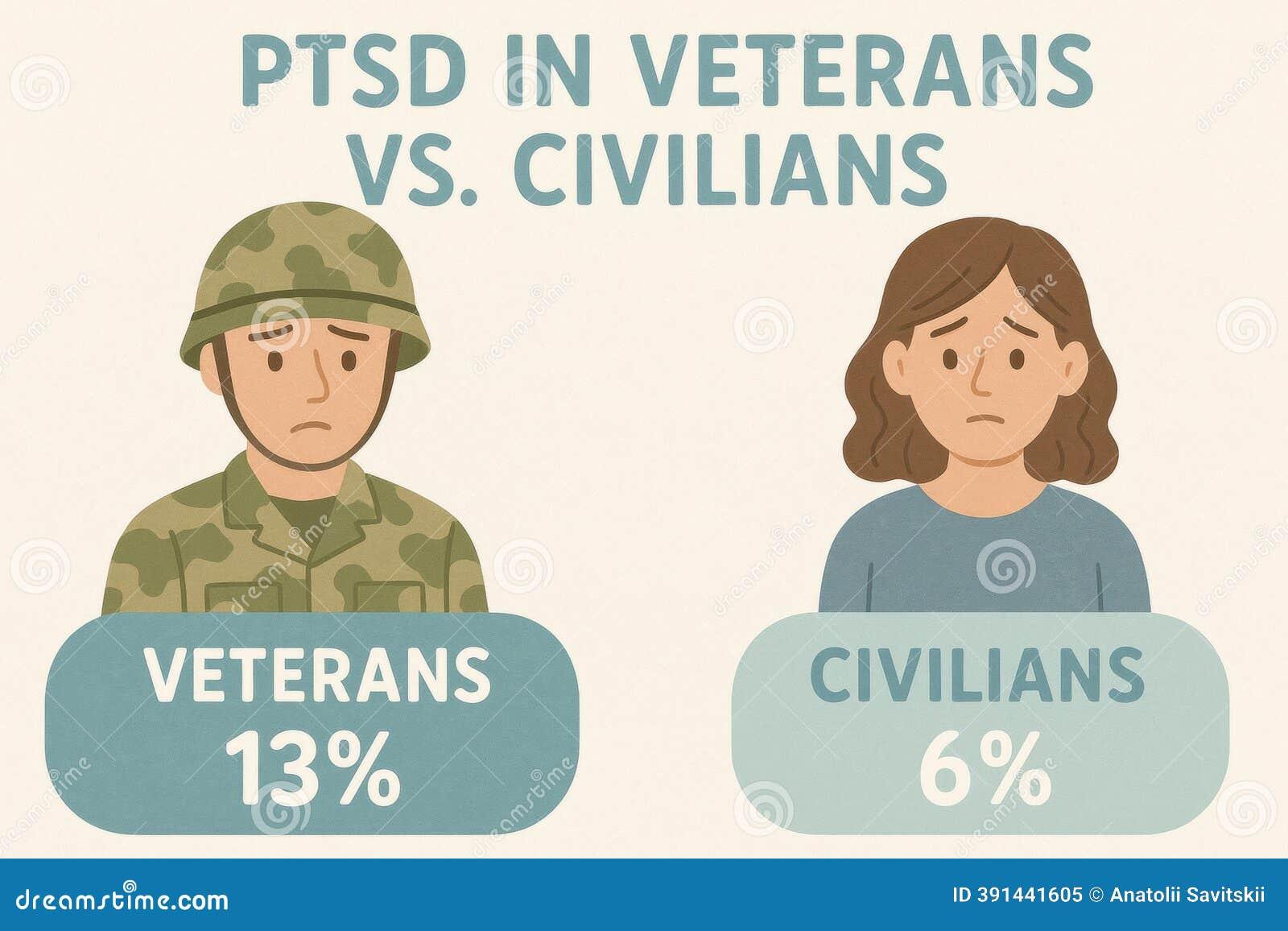
In 2018, a study by the National Epidemiologic Survey on Alcohol and Related Conditions-III (NESARC-III) revealed a striking disparity: male military veterans reported a lifetime PTSD prevalence of 7.7%, compared to just 3.4% among civilian men. This gap, while often attributed to combat exposure, masks a more intricate reality. Veterans, even those who never saw combat, face unique occupational stressors—prolonged deployments, hierarchical pressures, and reintegration challenges—that amplify their vulnerability to trauma.
Dr. Katherine Magruder, a leading epidemiologist at the Medical University of South Carolina, notes that "the cumulative effect of military service extends beyond the battlefield, embedding stressors into daily life that civilians rarely encounter." Her findings align with data showing that non-combat-related traumas, such as sexual assault or severe accidents, contribute significantly to PTSD rates among veterans.
Compounding this, the transition to civilian life often strips veterans of the camaraderie and structured support systems that once buffered their stress, leaving them disproportionately exposed to the long-term effects of trauma.
Defining PTSD and Its Symptoms
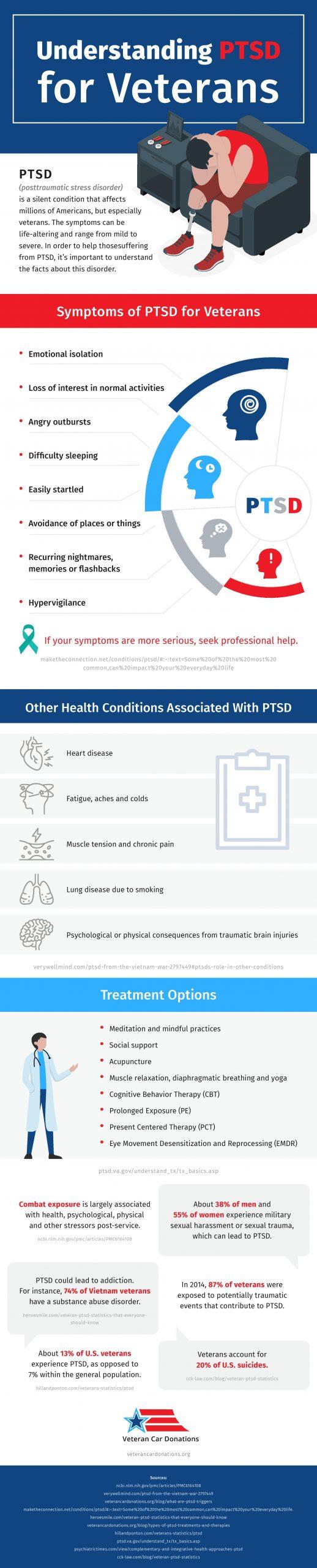
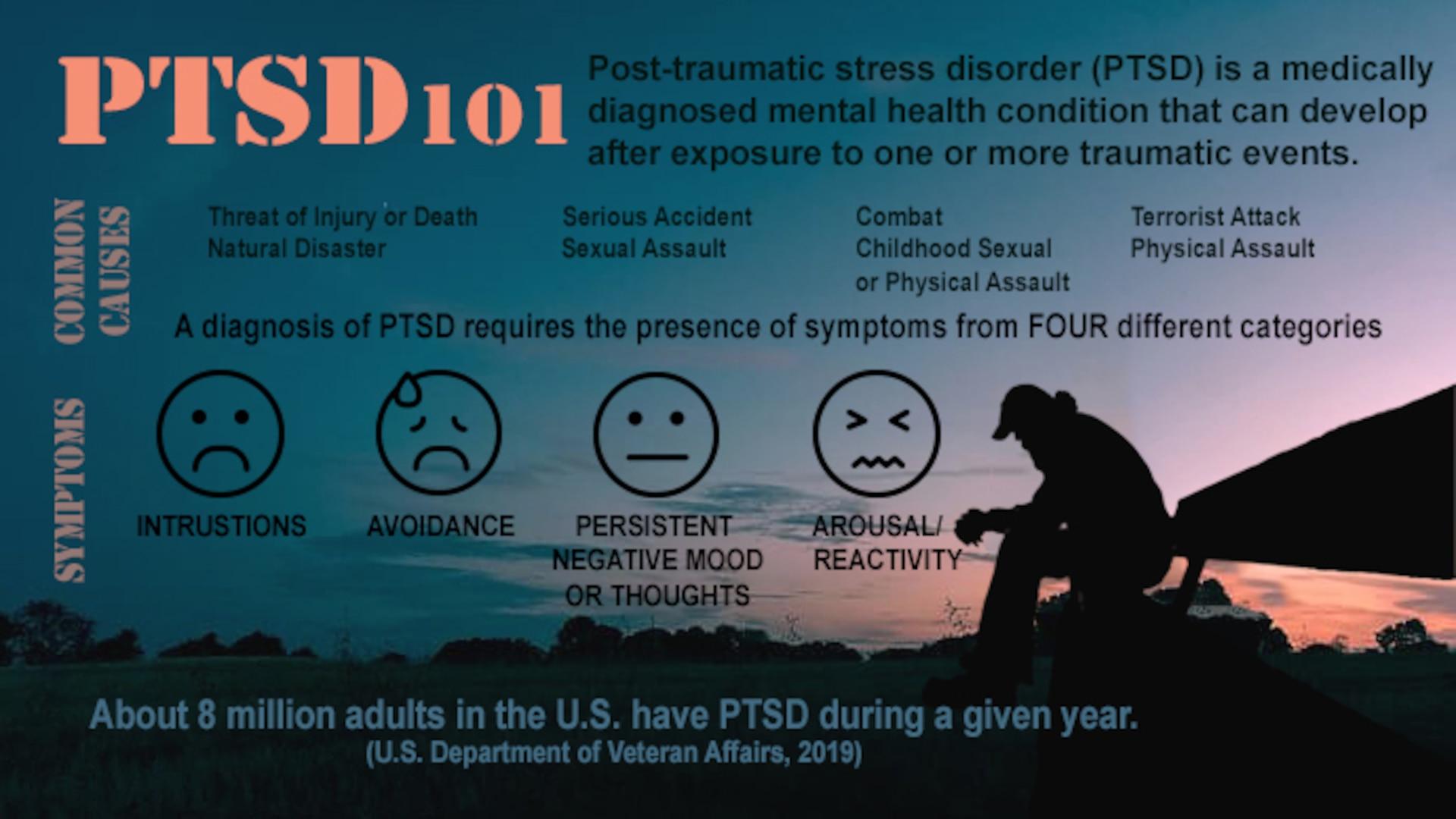
Posttraumatic Stress Disorder (PTSD) is often reduced to a checklist of symptoms—flashbacks, avoidance, hyperarousal—but this oversimplification obscures its dynamic nature. A critical yet underexplored aspect is the role of symptom evolution over time, particularly in veterans. Research by Bryant et al. (2017) in JAMA Psychiatry highlights that acute PTSD, characterized by intense reexperiencing symptoms, often transitions into chronic PTSD [1], [2], where emotional numbness and persistent fear responses dominate. This shift complicates diagnosis and treatment, as early interventions may not address the later, more entrenched symptom networks.
The diagnostic challenge is further compounded by comorbidities. A study by Kornfield et al. (2012) found that 43.9% of veterans with subsyndromal PTSD also suffered from depression, blurring the lines between primary and secondary conditions. This overlap necessitates a nuanced diagnostic approach that accounts for interrelated symptoms rather than isolating them.
"PTSD symptoms are not static; they morph in response to environmental and psychological factors," notes Dr. Rachel Yehuda, a leading trauma researcher.
Understanding these dynamics is essential for tailoring interventions. For instance, veterans with chronic PTSD may benefit more from therapies targeting emotional regulation, while acute cases might prioritize exposure-based techniques. This adaptive framework underscores the need for precision in both diagnosis and treatment.
Diagnostic Criteria and Symptomatology
The Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for PTSD provide a structured framework, yet their application often reveals significant limitations in real-world contexts [3], [4]. One critical issue is the static nature of these criteria, which fail to account for the fluid progression of symptoms over time. For instance, while the DSM emphasizes hallmark symptoms such as intrusive memories and hyperarousal, it does not adequately address how these may transition into more chronic manifestations like emotional detachment or cognitive impairments.
A comparative analysis of diagnostic approaches highlights this gap. Traditional checklist-based methods prioritize immediate symptom identification but often overlook subtler, evolving patterns. In contrast, longitudinal assessments, which track symptom progression over months or years, offer a more nuanced understanding. This distinction is particularly relevant for veterans, whose symptoms frequently shift from acute re-experiencing to persistent avoidance and numbing, influenced by environmental stressors and reintegration challenges.
"PTSD is not a static condition; its symptoms adapt to the individual's psychological and social environment," explains Dr. Rachel Yehuda, a leading expert in trauma research.
This dynamic nature underscores the importance of adaptive diagnostic tools. For example, the Department of Veterans Affairs has implemented periodic re-evaluations to capture symptom evolution [5], [2], improving both diagnostic accuracy and treatment outcomes. Such practices highlight the need for diagnostic frameworks that integrate temporal and contextual factors, ensuring more effective interventions.
Comparative Prevalence of PTSD in Veterans and Civilians
Male military veterans exhibit significantly higher lifetime PTSD prevalence (7.7%) compared to civilian men (3.4%), as reported by the National Epidemiologic Survey on Alcohol and Related Conditions-III. This disparity cannot be solely attributed to combat exposure. Instead, it reflects a broader spectrum of stressors, including prolonged deployments [4], [5], hierarchical pressures, and reintegration challenges, which amplify psychological vulnerability.
A critical factor is the nature of trauma exposure. While civilians often experience isolated traumatic events, veterans frequently endure cumulative stressors, such as witnessing death or sustaining injuries, which increase PTSD risk. Additionally, the military's structured environment may delay symptom recognition, as individuals often suppress distress to maintain operational readiness. This phenomenon, known as the "healthy warrior effect," complicates early diagnosis and intervention [2], [6].
Interestingly, veterans also face unique barriers to treatment. Studies indicate that male veterans delay seeking care longer than any other demographic, often due to stigma and fear of career repercussions. This delay exacerbates symptom severity, transforming acute PTSD into chronic conditions that are harder to treat.
These findings underscore the need for tailored diagnostic and therapeutic approaches that address the distinct experiences of veterans, moving beyond combat-centric models to encompass the full spectrum of military-related stressors.
Statistical Overview of PTSD Rates
The disparity in PTSD prevalence between male military veterans (7.7%) and civilian men (3.4%) reflects more than just differences in trauma exposure; it highlights the compounded effects of military-specific stressors [7], [6]. A critical factor is the cumulative nature of these stressors, which include not only combat-related events but also prolonged deployments, hierarchical pressures, and reintegration challenges. These elements create a unique psychological burden that is often underrepresented in civilian comparisons.
One overlooked dynamic is the role of delayed symptom recognition, influenced by the "healthy warrior effect." This phenomenon describes how military culture prioritizes resilience and operational readiness, leading many veterans to suppress or underreport symptoms until they become chronic. A study by Warner et al. (2011) demonstrated that anonymous surveys revealed significantly higher rates of PTSD symptoms compared to official post-deployment health assessments, underscoring the prevalence of underreporting.
Additionally, the transition from acute to chronic PTSD is more pronounced in veterans due to the interplay of environmental and psychological factors. For example, veterans exposed to multiple deployments often experience "allostatic load," a term describing the wear and tear on the body caused by chronic stress [4], [5]. This physiological mechanism exacerbates PTSD symptoms over time, making early intervention critical.
"PTSD in veterans is not just about combat; it’s about the accumulation of stressors that reshape the individual’s psychological and biological baseline," explains Dr. Rachel Yehuda, a leading trauma researcher.
These insights emphasize the need for diagnostic frameworks that account for the layered and evolving nature of PTSD in veterans, ensuring interventions address both immediate and long-term challenges.
Factors Contributing to Higher Prevalence in Veterans
One critical yet underexplored factor driving higher PTSD prevalence in veterans is the interplay between combat intensity and post-deployment social dynamics. While combat exposure is a well-documented risk, its effects are magnified by the absence of robust post-deployment support systems. Veterans often return to environments that lack the structured camaraderie of military life, creating a void that exacerbates psychological distress.
The concept of "allostatic load" provides a useful framework for understanding this phenomenon. Prolonged exposure to high-stress environments, such as multiple deployments, leads to cumulative physiological wear and tear. This biological mechanism not only heightens vulnerability to PTSD but also complicates recovery by impairing stress regulation systems. A meta-analysis published in PLOS One found that veterans with longer cumulative deployments exhibited significantly higher PTSD rates, underscoring the additive impact of sustained stress.
Compounding this [10], [11], the reintegration process often isolates veterans from their primary support networks. Unlike civilians, who may rely on consistent social structures, veterans face unique challenges in rebuilding connections. This isolation is particularly detrimental for those with preexisting vulnerabilities, such as prior trauma or low socioeconomic status, which further amplify PTSD risk.
"The transition from military to civilian life often dismantles the very support systems that buffered stress during service [8], [9]," explains Dr. Rachel Yehuda, a leading trauma researcher.
Addressing these factors requires a dual approach: enhancing post-deployment support and tailoring interventions to account for the cumulative nature of military stress. By integrating these elements, treatment frameworks can more effectively mitigate the long-term psychological burden faced by veterans.
Types of Traumatic Events Leading to PTSD
Combat-related trauma in military veterans often involves prolonged exposure to life-threatening situations, such as witnessing fatalities or enduring sustained attacks. A study by the Australian Defence Force identified that 66.2% of male veterans reported experiencing at least one traumatic event during service [12], [13], with many citing exposure to severe injuries or death as the most impactful [14], [8]. These events are compounded by the unpredictability and chronic nature of military operations, which amplify psychological strain.
In contrast, civilian trauma typically stems from isolated incidents like severe accidents or natural disasters. While these events are often singular, their intensity can lead to comparable PTSD outcomes. For instance, research from the National Center for PTSD highlights that civilians exposed to natural disasters exhibit a 20-30% PTSD prevalence, underscoring the profound impact of acute, high-stress events.
The divergence lies in the cumulative versus episodic nature of these traumas. Military personnel face repeated, layered stressors, while civilians often encounter singular, albeit severe, events. This distinction necessitates tailored diagnostic frameworks that account for the unique temporal and contextual dynamics of each group.
Combat-Related Trauma in Military Veterans
Combat-related trauma is distinguished by its cumulative and multifaceted nature [8], [9], which profoundly impacts the psychological resilience of military veterans. Unlike singular traumatic events, combat environments expose individuals to prolonged stressors, such as sustained firefights, the omnipresent threat of ambush, and witnessing the deaths of comrades. This repeated exposure disrupts the hypothalamic-pituitary-adrenal (HPA) axis, a critical component of the body’s stress response system, leading to heightened cortisol dysregulation and long-term psychological vulnerability.
A study published in PLOS One revealed that veterans with multiple deployments exhibited a 23% higher likelihood of developing PTSD compared to those with single deployments. This underscores the role of cumulative stress, which not only amplifies the severity of trauma but also impairs the brain's ability to process and recover from subsequent stressors. Furthermore, moral injuries—psychological wounds stemming from actions or inactions that violate deeply held ethical beliefs—compound the emotional toll, creating a unique subset of PTSD symptoms, including profound guilt and existential distress.
"PTSD in combat veterans is as much about the relentless, cumulative nature of combat stressors as it is about isolated incidents," explains Dr. Rachel Yehuda, a leading trauma researcher.
The practical implications of these findings are significant. Standard diagnostic frameworks often fail to capture the nuanced progression of PTSD in veterans, particularly the interplay between hypervigilance and emotional detachment. Tailored interventions, such as prolonged exposure therapy combined with moral injury-specific treatments, are essential to address these complexities. This approach not only improves diagnostic accuracy but also enhances therapeutic outcomes by targeting the unique stressors of combat environments.
Civilian Trauma: Accidents, Assaults, and Disasters
Civilian trauma often manifests through episodic yet profound events, such as severe accidents, assaults, or natural disasters. A critical yet underexplored aspect is the role of environmental and social context in shaping PTSD outcomes. Unlike military settings, where structured support systems and camaraderie can buffer psychological impacts, civilian environments frequently lack such protective mechanisms, leaving individuals more vulnerable to long-term distress.
Research highlights that the absence of immediate intervention following civilian trauma significantly increases the risk of chronic PTSD [17], [18]. For instance, a study by the National Center for PTSD found that individuals exposed to natural disasters who lacked access to psychological first aid were 40% more likely to develop persistent symptoms [12]. This underscores the importance of early, context-sensitive interventions tailored to the unique dynamics of civilian life.
One emerging framework involves integrating trauma-informed care into community health systems. This approach emphasizes recognizing the cumulative effects of repeated minor traumas, such as ongoing domestic violence or workplace harassment, which can mimic the layered stressors seen in combat veterans. By addressing these subtler patterns, practitioners can mitigate the risk of symptom escalation.
"The quiet persistence of everyday trauma can erode resilience just as effectively as a single catastrophic event [15], [16]," notes Dr. Rachel Yehuda, a leading trauma researcher.
Ultimately, the nuanced interplay between individual resilience, social support, and intervention timing highlights the need for adaptive strategies that bridge the gap between acute care and long-term recovery in civilian trauma cases.
Influence of Demographics and Service Era on PTSD
The interplay between demographics and service era reveals critical nuances in PTSD prevalence among male military veterans. For instance, veterans of Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) exhibit lifetime PTSD rates of 13–20%, significantly higher than those of Vietnam-era veterans, whose prevalence is estimated at 9–12%. This disparity reflects not only differences in combat intensity but also the cumulative stress of repeated deployments, a hallmark of modern military operations.
Demographic factors further shape PTSD outcomes. Younger veterans, particularly those aged 18–24 [4], [5], face the highest risk, as their underdeveloped coping mechanisms amplify the psychological toll of trauma [3]. Conversely, older veterans often exhibit delayed symptom onset, attributed to the "healthy warrior effect," where operational readiness masks early distress. Additionally, pre-service adversities, such as childhood maltreatment, increase PTSD susceptibility by up to 2.4 times, as shown in studies by the Department of Veterans Affairs.
These findings challenge the assumption that combat exposure alone drives PTSD. Instead, they underscore the importance of considering both the evolving nature of military service and individual vulnerabilities. Tailored interventions must address these intersecting factors, ensuring that treatment strategies evolve alongside the shifting demographics and operational demands of military populations.
Impact of Service Era and Combat Exposure
The evolution of military operations has fundamentally altered the psychological stressors faced by service members, with modern conflicts introducing unique dynamics that amplify PTSD risk. Veterans of Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) often endured multiple deployments with shorter recovery periods, a stark contrast to the single [5], [3], extended tours typical of Vietnam-era service. This operational tempo compounds stress through "allostatic load," a physiological concept describing the cumulative wear on the body’s stress response systems. Research from the National Center for PTSD indicates that veterans with three or more deployments are 27% more likely to develop chronic PTSD compared to those with fewer deployments.
Combat exposure itself has also shifted in nature. Modern warfare frequently involves asymmetrical threats, such as improvised explosive devices (IEDs) and urban combat, which create prolonged periods of hypervigilance. This contrasts with the more conventional, large-scale battles of earlier conflicts. A study published in PLOS One found that veterans exposed to IED attacks exhibited significantly higher rates of hyperarousal symptoms [19], [4], such as insomnia and heightened startle responses, compared to those in traditional combat scenarios.
"The unpredictability of modern combat environments imposes a psychological toll that extends far beyond the battlefield," explains Dr. Rachel Yehuda, a leading trauma researcher.
These findings underscore the need for adaptive treatment frameworks that address the evolving nature of combat stress. For instance, therapies targeting hypervigilance and emotional regulation may be more effective for OEF/OIF veterans, reflecting the distinct stress profiles shaped by their service era. This tailored approach ensures interventions remain relevant to the unique challenges of modern military operations.
Demographic Factors: Age, Gender, and More
Age and gender significantly influence PTSD vulnerability, shaping both symptom onset and progression [5], [4]. Younger veterans (18–24) exhibit the highest PTSD prevalence, often due to underdeveloped coping mechanisms and limited life experience in managing trauma. This contrasts with older veterans, who frequently experience delayed symptom emergence. The "healthy warrior effect," where operational readiness suppresses early distress, often masks symptoms in older cohorts, complicating later diagnoses. A study of OEF and OIF veterans revealed that those aged 18–24 were disproportionately diagnosed with PTSD compared to their older counterparts, underscoring the critical role of age in early intervention strategies.
Gender dynamics further complicate PTSD outcomes. While male veterans dominate military demographics, research highlights that women, even in smaller numbers [9], report higher PTSD rates post-combat. This disparity is often attributed to lower unit cohesion and higher pre-existing rates of depression among female service members. Additionally, men and women differ in emotional expression and help-seeking behaviors, influencing long-term recovery trajectories. For instance, men may underreport symptoms due to stigma, delaying treatment and exacerbating chronic conditions.
"Early-career service members are particularly susceptible due to underdeveloped resilience frameworks," notes Dr. Rachel Yehuda, a leading trauma researcher.
These findings emphasize the need for demographic-specific interventions. Tailoring support to younger veterans could focus on resilience training, while addressing gender-specific barriers may involve reducing stigma and enhancing access to care. Such nuanced approaches ensure that interventions align with the diverse needs of military populations.
FAQ
What are the key differences in PTSD prevalence between male military veterans and civilian men?
Male military veterans exhibit a significantly higher lifetime prevalence of PTSD compared to civilian men [20], with rates of 7.7% versus 3.4%, respectively. This disparity stems from the cumulative nature of military-specific stressors, including combat exposure [7], [6], prolonged deployments, and reintegration challenges. Veterans often face repeated traumatic events, such as witnessing death or sustaining injuries, which amplify psychological vulnerability. In contrast, civilian men typically encounter isolated traumatic incidents. Additionally, cultural stigma within military environments delays treatment-seeking among veterans, exacerbating chronic PTSD symptoms. These differences highlight the need for tailored diagnostic frameworks addressing the unique stressors experienced by male veterans.
How do combat-related and non-combat-related stressors contribute to PTSD in male veterans?
Combat-related stressors, such as exposure to life-threatening situations, witnessing fatalities, and sustaining injuries, are primary contributors to PTSD in male veterans. These experiences disrupt the hypothalamic-pituitary-adrenal (HPA) axis, heightening stress responses and psychological vulnerability. Non-combat-related stressors, including prolonged deployments, hierarchical pressures [9], [21], and reintegration challenges, further exacerbate PTSD risk. Additionally, events like severe accidents or military sexual trauma (MST) during service amplify emotional distress. The interplay of these stressors creates a cumulative psychological burden, making male veterans more susceptible to PTSD compared to civilians, who typically face isolated traumatic events rather than sustained, layered stress exposures.
What demographic factors, such as age and gender, influence PTSD rates in male military veterans compared to civilian men?
Age and gender significantly shape PTSD rates in male military veterans compared to civilian men. Younger veterans, particularly those aged 18–24, face heightened PTSD risk due to underdeveloped coping mechanisms and increased exposure to combat stressors [22], [20]. In contrast, older veterans often experience delayed symptom onset, influenced by the "healthy warrior effect," which masks early distress. Gender dynamics reveal that male veterans, despite higher PTSD prevalence than civilian men, are less likely to seek treatment due to stigma [6], [9]. Additionally, pre-service adversities [3], such as childhood trauma, further elevate PTSD susceptibility, underscoring the complex interplay of demographic factors in shaping mental health outcomes.
Why do male military veterans experience higher rates of PTSD than their civilian counterparts?
Male military veterans experience higher PTSD rates due to the cumulative and prolonged nature of military-specific stressors. Combat exposure, including life-threatening situations and witnessing fatalities [9], [23], significantly elevates psychological vulnerability. Non-combat factors, such as extended deployments, hierarchical pressures, and reintegration challenges, further compound stress. Unlike civilian men [24], [20], who typically face isolated traumatic events, veterans endure repeated exposures that disrupt stress regulation systems. Additionally, military culture often stigmatizes mental health issues, delaying treatment and exacerbating chronic symptoms. These unique occupational and environmental stressors create a layered psychological burden, distinguishing veterans’ PTSD prevalence from that of their civilian counterparts.
What role does reintegration into civilian life play in the development of PTSD among male veterans?
Reintegration into civilian life significantly influences PTSD development in male veterans by dismantling the structured support systems of military life. The loss of camaraderie and routine creates a void [21], [26], amplifying feelings of isolation and psychological distress [17], [25]. Veterans often struggle to adapt to civilian environments that lack the shared experiences and cohesion of military units. Additionally, challenges such as unemployment, strained family relationships, and societal stigma exacerbate emotional vulnerability. These factors, combined with pre-existing trauma, heighten the risk of chronic PTSD. Addressing reintegration stress through targeted support systems is crucial for mitigating its impact on veterans’ mental health outcomes.
References
PTSD in Veterans: Definition, Causes, Types, Symptoms, Effects, Treatment - Los Angeles Outpatient Center. Retrieved from https://laopcenter.com/mental-health/disorder/ptsd/veterans/
2 Diagnosis, Course, and Prevalence of PTSD | Treatment for Posttraumatic Stress Disorder in Military and Veteran Populations: Final Assessment | The National Academies Press. Retrieved from https://nap.nationalacademies.org/read/18724/chapter/4
History, Diagnostic Criteria, and Epidemiology - Treatment for Posttraumatic Stress Disorder in Military and Veteran Populations - NCBI Bookshelf. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK201095/
2 History, Diagnostic Criteria, and Epidemiology | Treatment for Posttraumatic Stress Disorder in Military and Veteran Populations: Initial Assessment | The National Academies Press. Retrieved from https://www.nap.edu/read/13364/chapter/4
2 History, Diagnostic Criteria, and Epidemiology | Treatment for Posttraumatic Stress Disorder in Military and Veteran Populations: Initial Assessment | The National Academies Press. Retrieved from https://nap.nationalacademies.org/read/13364/chapter/4
Post-traumatic Stress Disorder by Gender and Veteran Status - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC7217324/
(PDF) Post-traumatic Stress Disorder by Gender and Veteran Status. Retrieved from https://www.researchgate.net/publication/322168618_Post-traumatic_Stress_Disorder_by_Gender_and_Veteran_Status
Full article: PTSD in the military: special considerations for understanding prevalence, pathophysiology and treatment following deployment. Retrieved from https://www.tandfonline.com/doi/full/10.3402/ejpt.v5.25322
A Meta-Analysis of Risk Factors for Combat-Related PTSD among Military Personnel and Veterans | PLOS One. Retrieved from https://journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0120270
Prevalence Estimates of Combat-Related PTSD: A Critical Review - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC2891773/
Veteran and Military Mental Health Issues - StatPearls - NCBI Bookshelf. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK572092/
Post-Traumatic Stress Disorder and Blast Exposure in Active-Duty Military Service Members. Retrieved from https://www.mdpi.com/2673-866X/4/1/2
PTSD Statistics for US Veterans | Hill & Ponton, P.A.. Retrieved from https://www.hillandponton.com/resources/veterans-statistics-ptsd/
How Trauma Affects Military Personnel and Their Loved Ones. Retrieved from https://www.mcleanhospital.org/essential/military-trauma
Gender and Posttraumatic Stress Disorder Screening in the Military: A Measurement Study. Retrieved from https://trace.tennessee.edu/cgi/viewcontent.cgi?httpsredir=1&article=1892&context=utk_graddiss
PTSD History and Overview - PTSD: National Center for PTSD. Retrieved from https://www.ptsd.va.gov/professional/treat/essentials/history_ptsd.asp
https://d-scholarship.pitt.edu/31186/1/PaivanasT_MPHEssay_4_2017.pdf. Retrieved from https://d-scholarship.pitt.edu/31186/1/PaivanasT_MPHEssay_4_2017.pdf
The Effects of Childhood and Combat-Related Trauma on Psychological Outcomes in Veterans. Retrieved from https://scholarsrepository.llu.edu/cgi/viewcontent.cgi?article=1378&context=etd
Combat Exposure - PTSD: National Center for PTSD. Retrieved from https://www.ptsd.va.gov/understand/types/combat_exposure.asp
Post-traumatic Stress Disorder by Gender and Veteran Status - ScienceDirect. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0749379717304993
male vietnam veterans: Topics by Science.gov. Retrieved from https://www.science.gov/topicpages/m/male%2Bvietnam%2Bveterans
Gender, Population Type, and Coping as Predictors of PTSD Symptom Severity. Retrieved from https://scholarworks.sfasu.edu/cgi/viewcontent.cgi?article=1092&context=etds
It all adds up: Addressing the roles of cumulative traumatic experiences on military veterans - ScienceDirect. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0145213419304041
https://www.phoenixaustralia.org/wp-content/uploads/2022/08/Chapter-9-4.-Military-and-ex-military-personnel-1.pdf. Retrieved from https://www.phoenixaustralia.org/wp-content/uploads/2022/08/Chapter-9-4.-Military-and-ex-military-personnel-1.pdf
PTSD in U.S. Veterans: The Role of Social Connectedness, Combat Experience and Discharge. Retrieved from https://www.mdpi.com/2227-9032/6/3/102
Beyond war and PTSD_ The crucial role of transition stress in the lives of military veterans. Retrieved from https://www.tc.columbia.edu/media/centers-amp-labs/lte-lab/peered-review-journals/in-press_Mobbs--Bonanno_CPR.pdf