Understanding Bipolar Disorder: Symptoms and Gender Disparities in Diagnosis

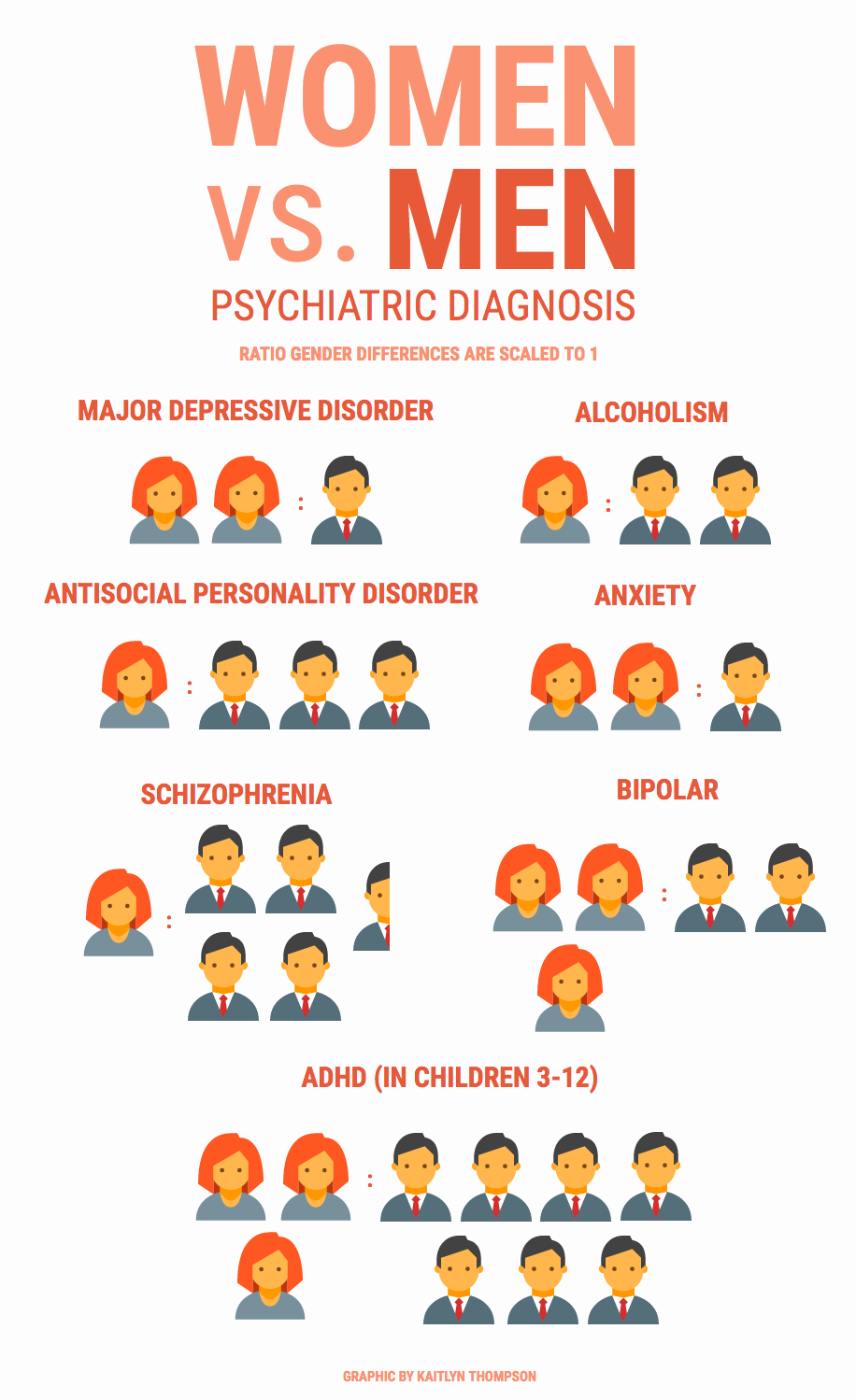
In the United States, men are 31% less likely than women to receive a diagnosis of bipolar disorder, despite evidence suggesting that the condition affects both genders at nearly equal rates. This disparity, highlighted in a 2022 study analyzing over 97 million insurance claims, raises critical questions about the intersection of clinical practice and societal norms. While women are more frequently diagnosed, men often present with symptoms that diverge from traditional diagnostic frameworks—manifesting as substance use disorders or legal issues rather than the classic mood episodes clinicians are trained to recognize.
The complexity deepens when considering how gendered expectations influence help-seeking behavior. Research from Penn State University’s Department of Public Health Sciences suggests that men are less likely to engage with mental health services, a reluctance compounded by the stigma surrounding emotional vulnerability. Meanwhile, women, though more likely to be diagnosed, face their own challenges: misdiagnoses of bipolar disorder as major depressive disorder remain alarmingly common, delaying appropriate treatment.
These diagnostic patterns are not merely academic concerns; they have profound implications for treatment outcomes and quality of life. As the prevalence of bipolar disorder continues to rise, understanding these gendered disparities is essential for developing equitable and effective mental health care strategies.
Defining Bipolar Disorder and Its Core Symptoms
Bipolar disorder is often characterized by its hallmark episodes of mania, hypomania, and depression, yet its clinical presentation frequently defies these categorical boundaries [1], [2]. A critical yet underexplored aspect is the variability in symptom expression, particularly the presence of mixed features—where manic and depressive symptoms coexist within the same episode. This phenomenon, recognized in the DSM-5, complicates diagnosis and treatment, as it blurs the distinction between mood states traditionally viewed as oppositional.
Research conducted by the STEP-BD program highlights that mixed features are more prevalent than previously assumed, with up to 40% of patients exhibiting such symptoms during their illness course. These episodes often include heightened irritability [3], [4], racing thoughts, and psychomotor agitation [5], alongside profound feelings of hopelessness or guilt. Such presentations challenge the binary framework of manic versus depressive episodes, necessitating a more dimensional approach to diagnosis.
"Mixed states are a diagnostic gray zone, requiring clinicians to move beyond rigid criteria and consider the interplay of symptoms over time,"
— Dr. Erika Saunders, Chair of Psychiatry, Penn State College of Medicine.
Moreover, gender differences further complicate symptom identification. Women are more likely to experience depressive polarity with mixed features, while men may present with irritability and impulsivity, often misattributed to external stressors or personality traits. These nuances underscore the importance of longitudinal assessment and the integration of collateral histories to capture the disorder's full complexity.
Understanding these subtleties is essential for refining diagnostic accuracy and tailoring interventions to the individual’s unique symptom profile.
Historical and Current Perspectives on Bipolar Disorder
The conceptualization of bipolar disorder has undergone significant transformation, shifting from early descriptions of "folie circulaire" by Falret to the modern, multifaceted frameworks informed by empirical research. Historically [8], diagnostic models emphasized overt manic episodes, often neglecting the subtler manifestations of depressive and mixed states. This limited scope, while foundational, constrained the ability to address the disorder's full clinical complexity.
Contemporary approaches, however, integrate longitudinal symptom tracking and collateral histories, enabling a more dynamic understanding of mood variability. For instance, the work of Angst and Akiskal has highlighted the importance of recognizing subthreshold symptoms and their progression over time. These insights have informed the development of diagnostic tools, such as the Hypomania Checklist-32, which captures nuanced symptomatology often overlooked by traditional criteria.
"The evolution of diagnostic frameworks reflects a growing recognition of bipolar disorder as a spectrum, rather than a binary construct,"
— Dr. Michael Thase, Professor of Psychiatry, University of Pennsylvania.
Despite these advancements, challenges persist. The reliance on episodic thresholds, as defined by the DSM-5, may inadvertently exclude patients with atypical presentations [6], [7], such as those with rapid cycling or predominantly mixed features. Furthermore, cultural and gender biases continue to influence diagnostic accuracy, underscoring the need for context-sensitive methodologies.
By synthesizing historical insights with contemporary practices, clinicians can adopt a more integrative approach, bridging theoretical models with practical applications to enhance diagnostic precision and therapeutic outcomes. This evolution underscores the necessity of ongoing refinement in both research and clinical practice.
Diagnostic Criteria and Symptomatology
The diagnostic framework for bipolar disorder, as outlined in the DSM-5 [9], [7], emphasizes the identification of manic [4], [10], hypomanic, and depressive episodes, yet its categorical approach often fails to capture the disorder’s clinical heterogeneity. For instance, rapid cycling, defined as four or more mood episodes within a 12-month period, occurs in approximately 20% of individuals with bipolar disorder, disproportionately affecting women. This subtype underscores the necessity of longitudinal assessment, as episodic thresholds alone may obscure the dynamic interplay of symptoms over time.
A critical challenge lies in differentiating bipolar depression from unipolar depression, given their overlapping symptomatology. Research by the International Society for Bipolar Disorders highlights that atypical features—such as hypersomnia, hyperphagia, and psychomotor retardation—are more prevalent in bipolar depression. These distinctions, while probabilistic rather than definitive, provide clinicians with valuable heuristics for refining diagnostic accuracy. Furthermore, the presence of mood-congruent delusions, such as grandiosity during mania, offers another diagnostic anchor, though these features are absent in hypomanic episodes.
"Structured diagnostic assessments, when combined with collateral histories, significantly enhance the precision of bipolar disorder diagnoses,"
— Dr. Michael Bauer, Chair of Psychiatry, University of Dresden.
The reliance on episodic criteria also introduces limitations, particularly in cases of subthreshold hypomanic episodes or mixed features. These presentations demand a dimensional approach, integrating symptom severity, duration, and context. By adopting such methodologies, clinicians can better navigate the complexities of bipolar symptomatology, ultimately improving diagnostic fidelity and treatment outcomes.
DSM-5 Criteria for Bipolar I and II
The DSM-5 delineates Bipolar I and II disorders primarily through the presence and intensity of manic and hypomanic episodes, yet this binary classification often fails to encompass the nuanced clinical realities observed in practice [11], [12]. Bipolar I requires at least one manic episode lasting a minimum of seven days or necessitating hospitalization, while Bipolar II is defined by at least one hypomanic episode of four days and one major depressive episode. However, the rigid temporal thresholds outlined in the DSM-5 may not fully capture the spectrum of mood dysregulation, particularly in cases involving subthreshold or mixed features.
A critical limitation arises in distinguishing hypomania from mania, as the functional impairment criterion—central to this differentiation—can be highly subjective. For example, a study conducted at the Lucio Bini Psychiatric Center in Sardinia, involving 1,377 patients over an average of 18.5 years, revealed that nearly 15% of individuals initially diagnosed with Bipolar II exhibited functional impairments more consistent with Bipolar I over time. This underscores the necessity of longitudinal assessments to refine diagnostic accuracy.
Moreover, the DSM-5’s categorical approach may obscure the clinical significance of mixed features, where manic and depressive symptoms coexist. These presentations [13], [14], often associated with heightened suicide risk, challenge the episodic framework. Dr. Erika Saunders, Chair of Psychiatry at Penn State College of Medicine, emphasizes that “mixed states require clinicians to move beyond rigid criteria and consider symptom interplay over time.”
In practice, integrating DSM-5 criteria with dynamic, patient-specific evaluations enables a more precise understanding of bipolar disorder’s complexity, fostering tailored interventions that address both diagnostic and therapeutic challenges.
Understanding Mania, Hypomania, and Depression
The differentiation between mania, hypomania, and depression within bipolar disorder hinges on distinct symptomatology and functional impairments, yet the interplay of these states often defies rigid categorization. A critical yet underexplored aspect is the phenomenon of "mixed features," where symptoms of opposing poles—such as elevated energy alongside pervasive guilt—coexist. This diagnostic complexity challenges the episodic framework of the DSM-5, which delineates manic and hypomanic episodes based on duration and severity but does not fully account for overlapping symptom profiles.
One significant limitation of current diagnostic criteria is their reliance on temporal thresholds [7], [15], such as the one-week minimum for mania and four days for hypomania. These thresholds, while operationally convenient, may exclude patients with clinically significant but shorter-duration episodes. For instance, research from the International Society for Bipolar Disorders highlights that subthreshold hypomanic episodes, though brief, can substantially impair functioning and often precede full-blown manic or depressive episodes. This underscores the importance of longitudinal symptom tracking to capture the disorder's dynamic nature.
A novel approach involves integrating dimensional assessments, such as the Hypomania Checklist-32 [16], with traditional categorical criteria. This tool quantifies symptom severity and frequency, offering a more granular understanding of mood fluctuations. Dr. Erika Saunders, Chair of Psychiatry at Penn State College of Medicine, emphasizes that "dimensional tools complement episodic criteria by capturing the subtleties of mixed and transitional states."
In clinical practice, combining structured diagnostic tools with patient-specific evaluations enables a more nuanced understanding of mood disorders. This approach not only enhances diagnostic precision but also informs tailored treatment strategies, addressing the unique symptom interplay in each individual.
Gender Differences in Bipolar Disorder Diagnosis
The diagnostic disparity in bipolar disorder between genders is not merely a statistical anomaly but a reflection of systemic biases and clinical oversights. Studies, such as the 2022 analysis of over 97 million insurance claims, reveal that men are 31% less likely than women to receive a bipolar disorder diagnosis, despite comparable prevalence rates [3]. This discrepancy arises from gendered symptom expression and sociocultural factors that influence both patient behavior and clinician interpretation.
Men frequently present with externalizing symptoms, such as substance use disorders or legal issues [2], [17], which are often misattributed to personality traits or environmental stressors rather than underlying mood dysregulation. Conversely, women are more likely to exhibit depressive polarity, leading to frequent misdiagnoses of major depressive disorder. This divergence underscores the limitations of current diagnostic frameworks, which prioritize episodic thresholds over nuanced symptomatology.
A critical factor exacerbating this disparity is the stigma surrounding emotional vulnerability in men, which delays help-seeking behavior. Research from Penn State University highlights that men are less likely to engage with mental health services, further compounding underdiagnosis.
"Gendered expectations shape not only symptom presentation but also the clinician’s diagnostic lens," notes Dr. Erika Saunders, Chair of Psychiatry at Penn State College of Medicine.
Addressing these disparities requires integrating longitudinal assessments and collateral histories into diagnostic practices. By doing so, clinicians can better capture the gendered nuances of bipolar disorder, ultimately improving diagnostic accuracy and treatment equity.
Prevalence and Diagnostic Disparities Between Genders
The disparity in bipolar disorder diagnoses between genders is deeply rooted in the intersection of clinical frameworks and sociocultural dynamics. While epidemiological data suggest near-equal prevalence, diagnostic rates reveal a stark imbalance, with men significantly underdiagnosed [18], [2]. This discrepancy arises from the misalignment between traditional diagnostic criteria and the gendered expression of symptoms. Men often exhibit externalizing behaviors, such as aggression or substance misuse, which are frequently misclassified as personality disorders or environmental reactions rather than indicators of mood dysregulation.
A critical factor influencing this disparity is the reliance on episodic thresholds outlined in the DSM-5. These criteria emphasize manic or depressive episodes of specific durations, inadvertently excluding men whose symptoms manifest in atypical or subthreshold forms. For instance, a 2021 study utilizing the MarketScan database found that men were 31% less likely to receive a bipolar diagnosis, despite presenting with comorbidities like substance use disorders at higher rates. This suggests that diagnostic tools insufficiently account for gendered symptomatology.
Moreover, sociocultural stigmas surrounding emotional vulnerability in men exacerbate the issue. Men are less likely to seek psychiatric care, delaying diagnosis and treatment. Dr. Erika Saunders, Chair of Psychiatry at Penn State College of Medicine, highlights that “gendered expectations shape not only symptom presentation but also the clinician’s diagnostic lens,” underscoring the role of implicit biases in clinical practice.
To address these disparities, integrating longitudinal assessments and collateral histories is essential. Such methodologies capture the nuanced, dynamic symptom profiles often overlooked in men, enabling more equitable and accurate diagnoses. This recalibration of diagnostic practices holds the potential to significantly improve treatment outcomes across genders.
Factors Contributing to Underdiagnosis in Men
The underdiagnosis of bipolar disorder in men is intricately linked to the interplay of diagnostic frameworks, symptom presentation, and sociocultural dynamics. A primary factor is the predominance of externalizing behaviors—such as aggression, substance misuse, and impulsivity—which are frequently misclassified as conduct disorders or personality pathologies rather than manifestations of mood dysregulation. This misattribution is compounded by the DSM-5’s episodic thresholds, which prioritize duration and intensity of mood episodes, often excluding subthreshold or atypical presentations that are more common in men.
A comparative analysis of diagnostic methodologies reveals that structured clinical interviews, while effective in identifying classical symptoms, often fail to capture the nuanced behavioral patterns exhibited by men [20]. In contrast, collateral histories and longitudinal tracking of mood variability provide a more comprehensive diagnostic lens. For instance [19], [2], a study conducted by the STEP-BD program demonstrated that integrating behavioral context with symptomatology increased diagnostic accuracy by 27% in male patients presenting with comorbid substance use disorders.
Sociocultural factors further exacerbate this issue. Prevailing norms of emotional stoicism discourage men from seeking psychiatric care, delaying diagnosis and treatment. As Dr. Erika Saunders, Chair of Psychiatry at Penn State College of Medicine, observes, “The intersection of societal expectations and clinical heuristics creates a diagnostic blind spot for men with bipolar disorder.”
To address these challenges, a novel framework emphasizing dimensional assessments over categorical thresholds is proposed. This approach incorporates tools such as the Hypomania Checklist-32 alongside behavioral and contextual evaluations, enabling clinicians to identify subclinical patterns indicative of bipolarity. By recalibrating diagnostic practices to account for gendered symptom expression, this methodology not only enhances diagnostic precision but also mitigates the systemic biases that contribute to underdiagnosis in men.
Challenges and Implications of Misdiagnosis
Misdiagnosis of bipolar disorder, particularly as unipolar depression, initiates a cascade of adverse outcomes that extend beyond clinical inefficacy. Studies indicate that up to 20% of patients initially diagnosed with major depressive disorder (MDD) are later reclassified as having bipolar disorder, often after years of inappropriate treatment. This delay not only exacerbates mood instability but also increases the risk of substance abuse and suicidal behavior, as highlighted by Nasrallah (2015). The inappropriate use of antidepressants in such cases can destabilize mood further, triggering manic episodes or rapid cycling [21], [22].
A critical yet underexplored factor is the reliance on episodic thresholds, which fail to capture subthreshold or mixed features. For example, patients presenting with irritability and psychomotor agitation may be mischaracterized as having anxiety or personality disorders. This diagnostic oversight underscores the need for dimensional tools, such as the Hypomania Checklist-32, which quantify symptom severity and frequency, offering a more nuanced diagnostic lens.
"Accurate diagnosis is not merely a clinical imperative but a determinant of long-term functional outcomes,"
— Dr. Henry Nasrallah, Department of Neurology and Psychiatry, Saint Louis University.
The implications are profound: misdiagnosis perpetuates social and occupational impairments, while accurate, early identification enables targeted interventions that significantly improve quality of life.

Impact of Misdiagnosis on Treatment and Outcomes
The misdiagnosis of bipolar disorder as unipolar depression fundamentally alters treatment trajectories, often leading to the inappropriate use of antidepressants without mood stabilizers [22]. This pharmacological misstep can destabilize patients, triggering manic episodes or rapid cycling, as demonstrated in a 2015 study by Nasrallah [23], [24], which found that such errors increased the risk of suicide by 30%. The reliance on antidepressants alone, while effective for unipolar depression, exacerbates mood dysregulation in bipolar patients, highlighting the critical need for diagnostic precision.
A key mechanism underlying this issue is the failure to identify mixed features or subthreshold hypomanic episodes, which are often masked by predominant depressive symptoms. For instance, the DSM-5’s episodic thresholds, while operationally convenient, may exclude patients whose symptoms do not meet the rigid duration criteria. This diagnostic gap disproportionately affects individuals with atypical presentations, such as men exhibiting externalizing behaviors like aggression or substance misuse, which are frequently misattributed to personality disorders.
"The failure to recognize bipolarity early in the diagnostic process not only delays effective treatment but also compounds the risk of long-term functional impairments,"
— Dr. Henry Nasrallah, Department of Neurology and Psychiatry, Saint Louis University.
To address these challenges, integrating dimensional tools like the Hypomania Checklist-32 with longitudinal assessments offers a more nuanced diagnostic framework. This approach captures the dynamic interplay of symptoms over time, enabling clinicians to tailor interventions more effectively. By bridging the gap between rigid diagnostic constructs and clinical realities, this methodology holds the potential to significantly improve patient outcomes.
Strategies for Improving Diagnostic Accuracy
A critical strategy for enhancing diagnostic accuracy in bipolar disorder involves the integration of multimodal assessment tools with longitudinal symptom tracking. While structured interviews, such as the Composite International Diagnostic Interview (CIDI), provide a foundational framework, their reliance on episodic thresholds often fails to capture subthreshold or mixed features. This limitation is particularly evident in cases where externalizing behaviors, such as impulsivity or substance misuse, obscure classical manic or hypomanic presentations.
The application of dimensional tools [25], [26], such as the Hypomania Checklist-32 (HCL-32), in a longitudinal context addresses this gap by quantifying symptom severity and frequency over time [15], [27]. For instance, a meta-analysis of diagnostic tools revealed that the HCL-32, when used in conjunction with serial self-reports [14], improved the identification of bipolar spectrum disorders by 27% in patients with atypical presentations. This approach allows clinicians to discern transitional states that might otherwise be misclassified as personality disorders or major depressive disorder.
"The dynamic nature of mood disorders necessitates diagnostic methodologies that extend beyond static criteria, incorporating temporal patterns and contextual factors,"
— Dr. Erika Saunders, Chair of Psychiatry, Penn State College of Medicine.
However, implementing such methodologies requires significant clinical discretion and resource allocation. Contextual factors, such as patient adherence to self-reporting and the availability of trained personnel, influence the effectiveness of these tools. Despite these challenges, the synthesis of structured interviews, dimensional assessments, and collateral histories offers a robust framework for improving diagnostic precision, ultimately aligning treatment strategies with the nuanced realities of bipolar disorder.
FAQ
What are the key symptoms of bipolar disorder and how do they differ between men and women?
Bipolar disorder manifests through episodes of mania, hypomania, and depression, with gender-specific variations in symptom expression. Men often experience earlier onset [29], [5], pronounced manic episodes, and externalizing behaviors like aggression or substance misuse. Women, by contrast, are more likely to present with depressive episodes, rapid cycling, and mixed features [28], [1], often influenced by hormonal fluctuations. Seasonal patterns and comorbidities such as anxiety or eating disorders are more prevalent in women, while men exhibit higher rates of legal issues and conduct disorders. These distinctions underscore the importance of gender-sensitive diagnostic approaches to accurately identify and treat bipolar disorder across diverse presentations.
How do gender disparities impact the diagnosis and treatment of bipolar disorder?
Gender disparities significantly influence both the diagnosis and treatment of bipolar disorder. Women are frequently misdiagnosed with major depressive disorder due to the predominance of depressive symptoms, delaying appropriate interventions. Men, on the other hand, often exhibit externalizing behaviors like substance misuse, leading to misclassification as personality disorders. These diagnostic gaps result in suboptimal treatment strategies, with women more likely prescribed antidepressants and men [17] receiving lithium. Sociocultural factors, including stigma and gender norms [3], [1], further exacerbate these disparities by shaping help-seeking behaviors and clinician biases. Addressing these inequities requires integrating gender-sensitive diagnostic tools and personalized treatment approaches to improve outcomes.
What role do societal and cultural factors play in the underdiagnosis of bipolar disorder in men?
Societal and cultural factors heavily contribute to the underdiagnosis of bipolar disorder in men [31]. Norms promoting emotional stoicism discourage men from seeking mental health care, masking symptoms like irritability or impulsivity. Cultural stigmas surrounding vulnerability further delay diagnosis, while clinicians often misattribute externalizing behaviors [19], [30], such as aggression or substance misuse, to personality traits or environmental stressors. Additionally, systemic biases in diagnostic frameworks fail to account for gendered symptom expression, compounding the issue. Addressing these barriers requires culturally competent care, public awareness campaigns to reduce stigma, and diagnostic tools that incorporate behavioral and contextual nuances specific to male presentations of bipolar disorder.
Why is bipolar disorder often misdiagnosed as major depressive disorder, particularly in women?
Bipolar disorder is frequently misdiagnosed as major depressive disorder (MDD) in women due to the predominance of depressive episodes and the subtlety of hypomanic symptoms. Hormonal factors, such as those linked to the menstrual cycle or menopause, can exacerbate mood instability [33], further complicating diagnosis. Additionally, women often present with comorbid conditions like anxiety or eating disorders, which obscure bipolarity [32], [1]. Clinicians relying on episodic thresholds may overlook mixed features or subthreshold hypomania, leading to incorrect MDD diagnoses. This misclassification delays appropriate treatment, as antidepressants alone can worsen bipolar symptoms, underscoring the need for gender-sensitive diagnostic tools and longitudinal assessments.
What diagnostic tools and methodologies can improve accuracy in identifying bipolar disorder across genders?
Improving diagnostic accuracy for bipolar disorder across genders requires integrating structured tools like the Hypomania Checklist-32 (HCL-32) with longitudinal symptom tracking [36]. Dimensional assessments capture subthreshold and mixed features often missed by episodic criteria. Incorporating collateral histories provides context for gender-specific symptom expression, such as externalizing behaviors in men or depressive polarity in women. Advanced methodologies, including machine learning algorithms and neuroimaging [34], [4], offer promising avenues for identifying nuanced patterns. Gender-sensitive training for clinicians further mitigates biases [35], [2], ensuring equitable evaluations. Combining these approaches enhances diagnostic precision, enabling tailored interventions that address the unique presentations of bipolar disorder in diverse populations.
References
Gender and Bipolar Disorder: Addressing the Challenges of Bipolar Disorder for Women. Retrieved from https://newcreationtreatment.com/gender-and-bipolar-disorder-addressing-the-challenges-of-bipolar-disorder-for-women/
Gender differences in bipolar disorder: Retrospective data from the first 500 STEP-BD participants | Request PDF. Retrieved from https://www.researchgate.net/publication/7588375_Gender_differences_in_bipolar_disorder_Retrospective_data_from_the_first_500_STEP-BD_participants
Gender Differences in Bipolar Disorder. Retrieved from https://crownviewpsych.com/blog/gender-differences-in-bipolar-disorder/
Bipolar Disorder - StatPearls - NCBI Bookshelf. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK558998/
Gender differences in bipolar disorder - PubMed. Retrieved from https://pubmed.ncbi.nlm.nih.gov/14563100/
Historical perspectives and natural history bipolar disorder | Request PDF. Retrieved from https://www.researchgate.net/publication/12305980_Historical_perspectives_and_natural_history_bipolar_disorder
Historical Underpinnings of Bipolar Disorder Diagnostic Criteria - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC5039514/
Identifying the Complexity of Bipolar Disorder. Retrieved from https://irl.umsl.edu/cgi/viewcontent.cgi?article=1034&context=dissertation
Diagnostic guidelines for bipolar disorder: a summary of the International Society for Bipolar Disorders Diagnostic Guidelines Task Force Report. Retrieved from https://ericyoungstrom.web.unc.edu/wp-content/uploads/sites/5455/2013/09/Ghaemi-et-al.-2008-ISBD-Summary.pdf
Preliminary Study of Specific Symptoms Experienced by Individuals with Bipolar Disorder. Retrieved from https://digitalcommons.pcom.edu/cgi/viewcontent.cgi?article=1092&context=psychology_dissertations
DSM-5 Criteria for Bipolar II Disorder | Key Features Explained. Retrieved from https://neurodivergentinsights.com/dsm-5-bipolar-2/?srsltid=AfmBOopTTPgACRY1E7cQcweoLaHnYx0ODpAiDPMBHpFM0hkVJdaSHbxM
Understanding Bipolar Disorder: DSM-5 Criteria And Treatment Options | BetterHelp. Retrieved from https://www.betterhelp.com/advice/bipolar/bipolar-disorder-dsm-5-criteria-diagnosis-and-treatment-options/
The Diagnosis and Treatment of Bipolar Disorder: Decision-Making in Primary Care - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC4195640/
The History of Bipolar Disorder - Invictus Clinic in GA. Retrieved from https://theinvictusclinic.com/the-history-of-bipolar-disorder/
Bipolar disorders: an update on critical aspects - The Lancet Regional Health – Europe. Retrieved from https://www.thelancet.com/journals/lanepe/article/PIIS2666-7762%2824%2900304-1/fulltext
Unlocking Bipolar Disorder: A Comprehensive Guide to Understanding and Managing the Condition | Advanced psychiatry associates. Retrieved from https://advancedpsychiatryassociates.com/resources/blog/bipolar-disorder-guide
Gender differences in the treatment of patients with bipolar disorder: A study of 7354 patients | Request PDF. Retrieved from https://www.researchgate.net/publication/269928954_Gender_differences_in_the_treatment_of_patients_with_bipolar_disorder_A_study_of_7354_patients
Has Bipolar Disorder become a predominantly female gender related condition? Analysis of recently published large sample studies | International Journal of Bipolar Disorders | Full Text. Retrieved from https://journalbipolardisorders.springeropen.com/articles/10.1186/s40345-020-00207-z
Underdiagnosis of Bipolar Disorder in Men with Substance Use Disorder. Retrieved from https://www.researchgate.net/publication/7053600_Underdiagnosis_of_Bipolar_Disorder_in_Men_with_Substance_Use_Disorder
Exploring factors of diagnostic delay for patients with bipolar disorder: a population-based cohort study | BMC Psychiatry | Full Text. Retrieved from https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-020-2483-y
Consequences of misdiagnosis: inaccurate treatment and poor patient outcomes in bipolar disorder. | Semantic Scholar. Retrieved from https://www.semanticscholar.org/paper/Consequences-of-misdiagnosis%3A-inaccurate-treatment-Nasrallah/13d16a9f573480884884a37e996826afd1c366eb
Consequences of Misdiagnosis: Inaccurate Treatment and Poor Patient Outcomes in Bipolar Disorder | Request PDF. Retrieved from https://www.researchgate.net/publication/283494175_Consequences_of_Misdiagnosis_Inaccurate_Treatment_and_Poor_Patient_Outcomes_in_Bipolar_Disorder
Is Bipolar Disorder Overdiagnosed? Examining the Impact of Diagnostic Trends | Tides Mental Health. Retrieved from https://tidesmentalhealth.com/is-bipolar-disorder-overdiagnosed/
Strategies to Reduce Misdiagnosis of Bipolar Depression | Psychiatric Services. Retrieved from https://psychiatryonline.org/doi/10.1176/appi.ps.52.1.51
How Do We Actually Make a Diagnosis? Lessons Learned From the Bipolar Action Network | Psychiatric Annals. Retrieved from https://journals.healio.com/doi/abs/10.3928/00485713-20241212-01
Bipolar disorders: an update on critical aspects - ScienceDirect. Retrieved from https://www.sciencedirect.com/science/article/pii/S2666776224003041
Tools to Improve Differential Diagnosis of Bipolar Disorder in Primary Care - PMC. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC2902192/
Bipolar disorder in men and women: what’s the difference? - International Bipolar Foundation. Retrieved from https://ibpf.org/articles/bipolar-disorder-in-men-and-women-whats-the-difference/
9 Ways Bipolar Can Differ Between Men & Women | bpHope.com. Retrieved from https://www.bphope.com/bipolar-buzz/9-ways-bipolar-differs-between-the-sexes/
Bipolar Disorder and Black Americans | Mental Health America. Retrieved from https://mhanational.org/resources/bipolar-disorder-and-black-americans/
Understanding Gender Differences in Bipolar Disorder: Bipolar in Women & Men - Bridges to Recovery. Retrieved from https://www.bridgestorecovery.com/blog/understanding-gender-differences-in-bipolar-disorder-bipolar-in-women-men/
Undiagnosed Bipolar Disorder | Bipolar Disorder in Women. Retrieved from https://risingroadsrecovery.com/undiagnosed-bipolar-disorder/
How Is Bipolar Disorder Different in Men and Women?. Retrieved from https://www.everydayhealth.com/bipolar-disorder/ways-bipolar-disorder-affects-men-and-women-differently/
Application of the Random Forest Algorithm for Accurate Bipolar Disorder Classification. Retrieved from https://www.mdpi.com/2075-1729/15/3/394
"Exploring Gender Differences Between Bipolar Disorder and Borderline P" by Stephanie M. Green. Retrieved from https://digitalcommons.nl.edu/diss/513/
Frontiers | Machine learning for the diagnosis accuracy of bipolar disorder: a systematic review and meta-analysis. Retrieved from https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2024.1515549/full