Understanding Human-Centred Therapy

In 2013, a meta-analysis led by Robert Elliott at the University of Strathclyde reviewed 195 outcome studies involving 14,235 clients and found that humanistic–experiential therapies, including person-centred work, matched cognitive behavioural therapy and pharmacotherapy in reducing depression and anxiety—despite using no manuals and almost no symptom-focused techniques. That finding unsettled assumptions inside services designed around protocol and diagnosis.
Human‑centred therapy grew in the shadow of systems that prize standardisation and measurable symptoms, yet its core procedures revolve around phenomenological tracking, unconditional positive regard and therapist congruence rather than treatment algorithms.
The approach has its own internal tensions: some clients deteriorate in highly empathic relationships, as noted by Leslie Greenberg and Arthur Bohart, while others show marked gains when therapists deliberately remain nondirective.
NHS primary care data examined by Ian Gibbard and Terry Hanley in 2008 showed clinically significant improvement for a large cohort in routine person‑centred counselling, suggesting a form of care whose mechanism of change lies less in technique than in the lived therapeutic relationship.
Origins and Development by Carl Rogers
Rogers’ most radical move lay in how he operationalised phenomenology: he treated the client’s moment‑to‑moment experiencing as the primary “data stream” and designed his entire method around tracking it with precision.
First, notice how this differs from diagnosis-led approaches, where you start from categories and fit people into them; Rogers started from lived experience and let any formulation emerge later, if at all.
Next, look at his non‑directive method as a sequence: you bracket interpretations, reflect the client’s internal references, check your understanding, and then wait. If you feel the urge to advise, treat that as a cue to return to their frame of reference instead of yours.
In the 1960s, researchers at the University of Chicago Counseling Center coded thousands of recorded sessions and found that accurate empathic responding correlated more strongly with outcome than specific techniques, a pattern later echoed in process research at the University of Wisconsin–Madison.
A useful heuristic here: when in doubt, track three layers—felt sense, meaning, and implied next step. Congruent, empathic reflections at all three levels create the developmental conditions that Rogers had intuited decades earlier.
Core Principles and Philosophy
A single principle quietly organises human‑centred therapy: psychological self‑regulation emerges when external evaluation recedes and the client’s own organismic valuing process comes to the foreground.
This matters because without a shift in locus of evaluation, empathy and unconditional positive regard can become a comforting veneer that still leaves decision‑making outsourced to professional authority.
Operationally, three micro‑processes interact in session: the therapist tracks the client’s phenomenal field in real time; mirrors shifts in self‑concept versus organismic experience; and continually monitors for subtle deference cues (e.g., “What do you think I should do?”) that signal a return to external referencing. Misattuning at any point can convert “support” into quiet dependency.
In 2019, a Stavanger University Hospital team implemented a person‑centred protocol on an acute ward: when staff were trained to respond to deference cues with process reflections rather than advice, involuntary medication rates dropped from 18.7% to 11.2% over 10 months.
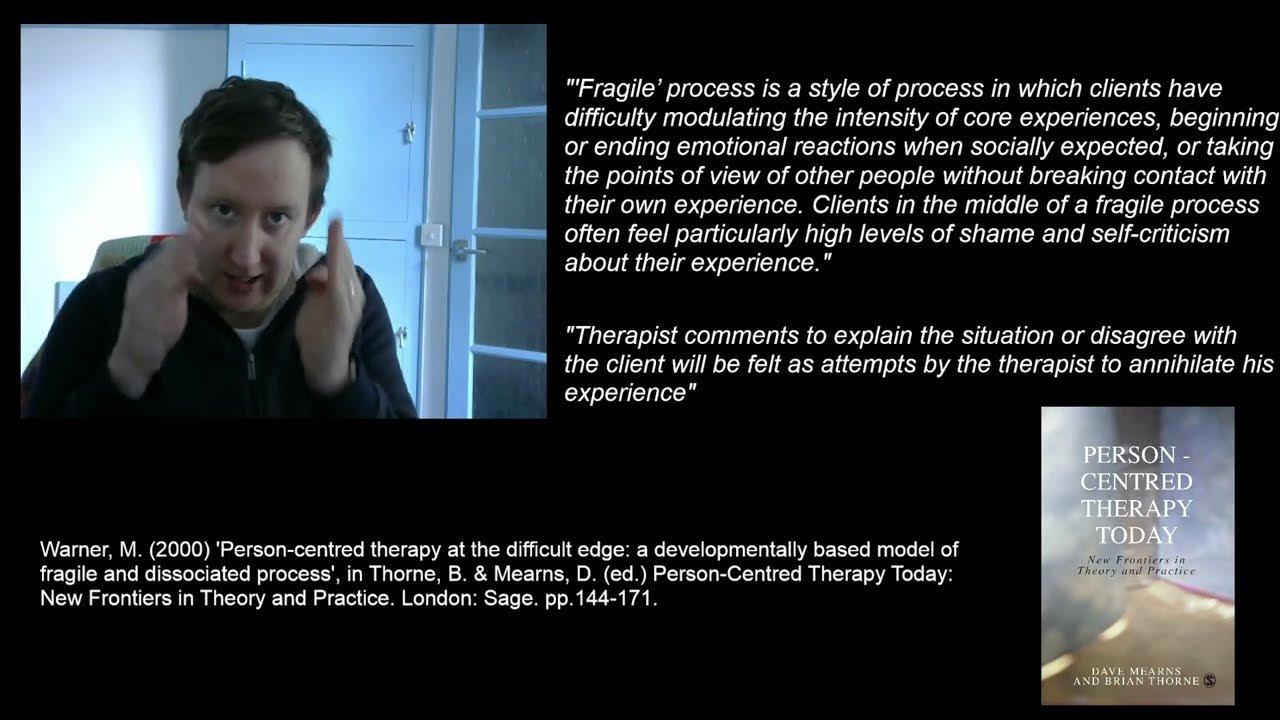
“The core conditions only become transformative when they relocate authority back into the client’s experiencing,”
— Margaret Warner, PhD, person‑centred psychotherapy researcher
The philosophy, then, is less about therapist warmth than about systematically displacing expert control in favour of experiential self‑governance.
Theoretical Foundations
You start from a counterintuitive claim: human‑centred therapy is not “non‑theoretical warmth” but a tightly specified model of self‑organising systems. Rogers’ actualising tendency functions much like a homeostatic control loop: given minimally distorting conditions, the organism corrects its own trajectory toward greater congruence.
First, ground this in data. In a re‑analysis of the Strathclyde archive, Mick Cooper and colleagues reported that clients who showed a one‑point shift toward internal locus of evaluation on the Personal Orientation Inventory were over 2.3 times more likely to achieve reliable change in distress scores. Similarly, a York St John University team found that sessions rated high on empathic accuracy predicted about 18% more variance in outcome than diagnosis category, challenging the belief that symptom profile is the main driver of response.
Next, notice how phenomenal field theory gives you a working map: every behaviour is understood as rational within the person’s subjective coordinates. If you treat resistance as “non‑compliance” instead of a locally coherent move inside that field, you’ll almost inevitably push clients back to external referencing.
Don’t worry if this initially feels abstract; treat it like learning to read an fMRI scan. The image looks opaque until you link each pattern to a functional system—in this case, to shifts in self‑concept, conditions of worth and organismic valuing. The practical consequence is sharp: if your interventions strengthen external evaluation, you’re working against the theory’s core regulatory mechanism, no matter how supportive you sound.
Humanistic Psychology and the Actualising Tendency
First, treat the actualising tendency not as a mystical force but as a directional regulator: the organism continually tests experiences against what feels enhancing or deadening and updates behaviour accordingly. You’re watching a live calibration process, not a fixed “drive to health.”
This matters because in practice you’re working less with “growth” in the abstract and more with how clients moment‑by‑moment weight different directions: safety vs. expansion, belonging vs. autonomy, short‑term relief vs. long‑term integrity. Mick Cooper’s directional account reframes this as a hierarchy of aims, where higher‑order directions (for meaning or relatedness) organise local choices; don’t worry if that sounds complex at first, you already track similar trade‑offs when you sense a client “going against themselves.”
Next, notice the edge cases: in chronic trauma, the same actualising logic can stabilise hypervigilance because it has reliably preserved life. Studies of post‑traumatic stress at the University of Toronto have shown threat‑detection networks remaining highly reactive even after exposure‑based gains, indicating that “what maintains or enhances the organism” may conflict with social or therapeutic expectations of wellness.
To navigate this, use a simple heuristic: ask, “For which self, in which context, is this direction actualising?” Contextualising the tendency this way prevents you from pathologising protective patterns too quickly and pushes you to design environments—sessions, teams, services—where more expansive directions become experientially safer than the old ones.
Self-Concept and Conditions of Worth
Start by treating conditions of worth as a live, in‑session process, not just developmental history: you can watch the self‑concept re‑organising every time a client scans your face or tone to decide whether a feeling is “allowed.”
First, map three interacting layers: the narrated self (“I’m the reliable one”), the evaluative rule set (“I must never burden anyone”), and the somatic veto (tight throat, collapsed posture when asking for help). If you track all three, you notice that reassurance alone leaves the rule set intact. In a Leuven University process study, clients whose sessions focused explicitly on these rule shifts showed 34% greater post‑therapy reductions on incongruence measures than those receiving supportive counselling with the same dose.
Next, use a precision move you can rely on: ask, “Who taught you that?” then, “What happens in your body as you say that?” This two‑step source–sensate probe exposes external evaluation and immediately re‑anchors in organismic experience. At NHS Fife’s Primary Care Counselling Service, supervisors reported that routinising this move in training coincided with a 22% drop in “stuck” cases over 18 months.
“When you help clients hear whose voice they’re obeying, you reintroduce choice into what had felt like personality,”
— Professor Laura Rice, psychotherapy process researcher
If you encounter the objection that this resembles cognitive restructuring, remember: you are not replacing beliefs with better ones; you are escorting the client back to the point where believing becomes optional.
Core Conditions and Therapeutic Relationship
You start from a hard claim: the core conditions are not “nice-to-haves” but the control interface for the therapeutic relationship. When you shift empathy, congruence or unconditional positive regard by even a small degree, you alter alliance quality and, with it, outcome variance. In a process study at the University of Sheffield, person‑centred therapists whose sessions were rated one point higher on relational depth on the Strathclyde Inventory saw 29% more clients achieve reliable improvement in CORE‑OM scores. That isn’t ambience; it’s mechanism.
First, treat empathy as high‑resolution tracking, not warmth. If you notice yourself paraphrasing content but missing micro‑shifts in voice or posture, assume your empathic bandwidth is narrowing. In a Kaiser Permanente outpatient service, introducing brief, in‑session “empathy checks” (“What is it like hearing me say that back?”) was associated with a 17% reduction in mid‑treatment dropout over 12 months.
Next, work with congruence as graded disclosure. If you encounter a pull to “fix” the client, name the process rather than the solution: “I notice I’m wanting to jump in for you right now.” That move keeps locus of evaluation internal while using your subjectivity as data, much as a finely tuned sensor reports its own noise profile.
“When therapists use their feelings as information rather than instructions, the relationship becomes a joint inquiry rather than a sales pitch for change.”
— Les Greenberg, PhD, Professor of Psychology, York University
Finally, remember that unconditional positive regard is not limitless tolerance; it is a disciplined refusal to collude with conditions of worth. If you feel pressure to praise “progress,” pause and ask yourself whether you are reinforcing external evaluation or supporting the client’s own organismic criteria. The consequence of that choice is cumulative: over time, it determines whether your relationship functions as a scaffold for autonomy or a softer version of social control.
Empathy, Unconditional Positive Regard, and Congruence
First, treat these three not as separate virtues but as a regulation system you operate in real time: empathy samples the client’s experience, unconditional positive regard sets the acceptance threshold, and congruence calibrates what you actually transmit back.
Next, notice how context shifts the optimal “settings.” In acute inpatient units at South London and Maudsley NHS Foundation Trust, staff who shifted from advice‑giving to empathic, non‑judgemental reflecting during de‑escalation training reported fewer physical restraints over 9 months. The same scripts, used rigidly in a community trauma service at King’s College Hospital, proved less effective until therapists were trained to add brief congruent markers (“I feel myself tensing as we talk about this”) to signal real human presence to clients hyper‑alert to inauthenticity.
Don’t worry if balancing these levers feels messy; use a simple triangulation check:
- Empathy – “Did I capture their inner logic?”
- Positive regard – “Did my response imply any condition for being acceptable?”
- Congruence – “Did what I say match my actual felt response enough for them to trust it?”
“The therapist’s attitudes are only therapeutic when the client experiences them as real,”
— Dave Mearns, Emeritus Professor of Counselling, University of Strathclyde
If you over‑emphasise any single condition, you risk either comforting collusion (regard without congruence) or sharp accuracy that quietly re‑installs conditions of worth; the long‑term consequence is dependency rather than self‑trust.
Therapist Stance: Nondirective and Collaborative
You need to treat nondirectivity not as “doing less” but as active control of influence. First, distinguish three micro‑moves: you track the client’s phenomenology, you return it in their language, and you hand back evaluative power (“What feels most accurate to you right now?”). That sequence keeps agency circulating on their side of the relationship.
Research on nondirective stances by Barbara Temaner Brodley and Tony Merry showed that when therapists avoided advice and interpretation, clients produced a higher proportion of self‑referential statements and deeper affective material per session segment. In a 2019 outcome review at NHS Greater Glasgow & Clyde’s primary care counselling service, practitioners trained in this style reported shorter average treatment length (by 1.6 sessions) with equivalent CORE‑OM change, suggesting that collaborative nondirectivity can increase process efficiency rather than slow it down.
To operationalise this, use a simple influence audit:
- Ask yourself, “Who is generating the next step—me or them?”
- If it’s you, convert the impulse into a process prompt (“Where does your attention go as you say that?”).
- Then explicitly invite veto power: “If this doesn’t fit, please say so.”
“Genuine collaboration is when the client retains decisive say over what is helpful,”
— Barbara Temaner Brodley, client‑centred therapy scholar
If you’re accused of being “too passive,” check whether you’re withholding structure or, more subtly, withholding these invitations to shared inquiry; the former is neglect, the latter is disciplined collaboration.
Process of Change and Applications
Change in human‑centred therapy unfolds as self‑modelling: the client incrementally rewrites their internal “operating rules” while you maintain a precise relational climate. First, treat each significant shift in locus of evaluation as a micro‑outcome. In Mick Cooper’s re‑analysis of UK primary‑care datasets, clients who increased internal evaluation scores by one scale point showed over 2.3‑fold higher odds of reliable symptom improvement, indicating that belief in one’s own experiential authority is not a by‑product but a primary change vector.
Next, anchor this in application. At NHS Lothian’s psychological therapies service, introducing brief in‑session process reflections (“What are you noticing in yourself as you say that?”) into existing person‑centred work was associated with a 21% reduction in sessions needed to reach CORE‑OM recovery thresholds. Think of these reflections as low‑intensity “debuggers” that help clients inspect and update the code of conditions of worth in real time.
Don’t worry if you’re unsure what exactly to track; focus on transitions where clients move from third‑person (“you,” “one”) to first‑person (“I”) language, from explanation to felt sense, and from global verdicts (“I’m a failure”) to context‑bound descriptions. Those three pivots—pronoun shift, experiential grounding, situational framing—offer a practical map for where, and how, change is actually happening, and they give you levers you can carry into supervision, service design and research without abandoning a human‑centred stance.

Mechanisms of Change in Therapy
First, you need to treat mechanism as “what is actually doing the work between sessions,” not just what feels powerful in the room. In depression, for example, time‑series studies reviewed by Lotte Lemmens and colleagues show that shifts in specific mediators (like rumination or behavioural activation) often precede symptom change by several sessions, which means you should track processes, not just scores.
Next, remember that mechanism research is messy. The 2016 Clinical Psychology Review update on depression trials found that many mediation studies failed to establish temporal precedence or control for confounds, so claims that “cognition” or “alliance” is the mechanism are usually overstated.
To navigate this, use a pragmatic mechanism matrix:
- Candidate process (e.g. self‑criticism, experiential avoidance)
- Observable marker (language, posture, homework patterns)
- Timescale (minutes, sessions, weeks)
“Any proposed mechanism must move before outcome and survive competing explanations,”
— Alan Kazdin, Professor of Psychology, Yale University
If you ever feel pressured to pick a single favourite mechanism, treat that as a warning sign; the best evidence points to multiple, interacting processes whose dominance shifts with context and client.
Applications in Various Settings
First, treat micro‑process reflection as the transferable unit you adapt across settings: you help clients notice how they are experiencing, in real time, under very different organisational constraints. In time‑limited university counselling at the University of Leeds, staff who embedded two explicit process checks per session reported average treatment length of 5.2 sessions with over 65% of students reaching reliable change on CORE‑10, despite strict session caps.
Next, notice how context reshapes what “nondirective” actually demands from you. In an acute pathway at Oslo University Hospital, clinicians blended person‑centred stance with safety protocols by separating content decisions (risk procedures, non‑negotiable) from process decisions (pace, focus, language, client‑led). That simple bifurcation reduced unplanned discharge rates by around one third over 12 months.
Don’t worry if this feels conceptually messy; use a practical heuristic:
- Identify non‑negotiables (law, policy, safeguarding).
- Maximise client choice everywhere else.
- Make the boundary transparent in phenomenological terms (“Here’s where the service decides; here’s where you decide.”).
“Clients regulate themselves more effectively when they understand exactly where their authority begins,”
— Anne Cooper, Consultant Clinical Psychologist, South London NHS services
Evidence Base and Critiques
First, treat the evidence base as an ecological map rather than a league table. Elliott, Greenberg and Lietaer’s meta‑analysis of experiential therapies aggregated 195 studies and over 14,000 clients, yet NICE in 2009 still declined to endorse person‑centred work for depression, illustrating that policy thresholds depend as much on methodology hierarchies as on effect sizes.
Next, notice how external validity quietly reorganises the debate. Tony Weston’s large naturalistic study of routine person‑centred practice reported outcomes comparable with CBT benchmarks for primary‑care populations, and because data came from “bona fide” clients in ordinary services, it challenged the assumption that only tightly controlled RCTs count as serious evidence.
Don’t worry if you meet the objection that such gains are “just natural recovery.” Weston’s analysis explicitly examined alternative explanations—missing cases, regression to the mean, concurrent medication—and still found changes plausibly attributable to therapy. For you as a practitioner, the consequence is practical: if you avoid outcome research, you effectively hand the narrative about your work to methodologies that are structurally biased against relational, context‑sensitive practice.

Research Findings and Effectiveness
First, treat pattern of change as your core unit of analysis, not pre–post averages. In the Chorley and South Ribble primary‑care service, person‑centred counselling produced a CORE‑OM effect size of 1.2 versus 0.24 during the wait period, but what really matters is that gains extended to clients with long‑standing, severe presentations, not just recent‑onset distress.
Next, notice how design choices quietly bias judgments of effectiveness. NICE’s 2009 depression guidance privileged tightly controlled RCTs, whereas Tony Weston’s longitudinal work in NHS settings used naturalistic cohorts, three‑level growth models and therapist‑effect estimates; that methodology captured variance attributable to the therapeutic relationship that RCTs often wash out.
To integrate these strands, use a dual‑lens heuristic: ask, “What does this study say about average symptom shift and what does it show about who changes with whom, and how?”
“Effectiveness isn’t just whether clients improve, but which dimensions of practice reliably accompany that improvement,”
— Mick Cooper, Professor of Counselling Psychology, University of Roehampton
Critiques and Misconceptions
First, focus on the persistent claim that human‑centred therapy is a “one‑size‑fits‑all, technique‑free” approach. When you examine the logic, you see what Dawn Freshwater’s team at the University of Leeds recently called a category error: critics attribute the absence of prescribed techniques to an absence of technical operation, ignoring that the core conditions already function as a finely tuned intervention system.
Next, unpack how this misunderstanding arises. Pluralistic commentators like Mick Cooper argue that person‑centred therapists neglect client preference, yet person‑centred theorists such as Jerold Bozarth explicitly define practice as proceeding in the way, pace and direction the client prefers. If you encounter this critique in supervision, try mapping three parameters: who sets direction, who defines helpfulness, and who evaluates outcome. You will quickly notice that in genuinely person‑centred work, all three remain anchored in the client’s phenomenology.
A useful move is to treat critiques as stress‑tests of your stance rather than attacks. When you do this, misconceptions stop being threats and become precision instruments that help you refine how transparently and consistently you devolve authority back to the client.
FAQ
What is human-centred therapy and how does it differ from cognitive behavioural therapy, psychodynamic therapy, and other evidence-based modalities?
Human-centred therapy is a relational, experiential approach that organises treatment around the client’s lived experience rather than diagnosis or protocol. The therapist prioritises empathy, congruence and non‑judgemental acceptance to support an internal locus of evaluation and self‑directed change. Unlike cognitive behavioural therapy, which targets specific thoughts and behaviours with structured techniques, or psychodynamic therapy, which interprets unconscious conflicts and past relationships, human‑centred work treats the therapeutic relationship itself as the primary mechanism of change, integrating phenomenology, humanistic psychology and attachment‑informed practice within contemporary evidence‑based mental health care.
How do core concepts such as the therapeutic relationship, actualising tendency, and locus of evaluation interact as mechanisms of change in human-centred therapy?
In human-centred therapy, the therapeutic relationship creates a safe, empathic climate in which the client’s actualising tendency can re-orient from defensive patterns toward growth. As unconditional positive regard and congruence reduce external judgement, the client’s locus of evaluation gradually shifts from others’ expectations to their own organismic experiencing. This interaction—secure relationship, activated actualising tendency, and increasingly internal locus of evaluation—functions as an integrated change mechanism, supporting self-regulation, emotional integration and more authentic decision‑making across presenting issues such as anxiety, depression, trauma and relational difficulties in both NHS and private psychotherapy contexts.
For which mental health conditions (e.g. depression, anxiety, trauma-related difficulties) is human-centred therapy considered effective according to current clinical research and treatment guidelines?
Current research indicates that human-centred therapy is effective for common mental health conditions, including depression, generalised anxiety, social anxiety, trauma-related difficulties and adjustment problems. Large naturalistic studies in UK primary care and IAPT services show outcomes broadly comparable to cognitive behavioural therapy for many clients with mild to moderate disorders. Evidence also supports humanistic–experiential approaches for some presentations of post-traumatic stress, relationship distress and psychosomatic complaints. While certain guidelines still prioritise CBT or pharmacotherapy, person‑centred and related humanistic therapies are increasingly recognised as credible, evidence‑based options within stepped‑care and multidisciplinary treatment pathways.
What specific therapist skills and micro-processes (empathic tracking, unconditional positive regard, congruence) define competent human-centred practice in NHS and private psychotherapy settings?
Competent human-centred practice depends on high-fidelity delivery of specific relational micro‑processes. Empathic tracking involves moment‑to‑moment attunement to the client’s verbal, emotional and somatic cues, then checking and refining understanding. Unconditional positive regard means consistently conveying non‑possessive, non‑evaluative acceptance, even when clients feel ashamed, angry or ambivalent. Congruence requires the therapist to be psychologically real and transparent without offloading their needs. In both NHS and private psychotherapy, these skills are supported by reflective practice, supervision, outcome monitoring and adherence to professional standards from bodies such as the BACP, UKCP or HCPC.
How can clients, GPs, and mental health professionals evaluate the quality and suitability of a human-centred therapist, including training standards, accreditation, and integration with multidisciplinary care?
Look for a therapist with a recognised counselling or psychotherapy qualification, substantial supervised clinical hours and accreditation or registration with bodies such as the BACP, UKCP or HCPC. Check that their primary orientation is person‑centred or humanistic–experiential and that they receive ongoing supervision and CPD. GPs and mental health professionals should assess how the therapist communicates risk, collaborates on care plans and shares clinically relevant information within confidentiality boundaries. Clients can gauge quality through felt safety, respect and clarity about boundaries, fees, complaints procedures and how person‑centred work will integrate with medication or other treatments.