Understanding Male Mental Health in Military Contexts: Barriers, Support Systems, and Long-Term Impact
In 2017, a study by the U.S. Department of Defense revealed that nearly 60% of active-duty military personnel who met the criteria for a mental health condition did not seek treatment. This statistic, while alarming, is only the surface of a deeper issue: the pervasive stigma and structural barriers that define mental health care in military contexts. For many service members, the fear of being perceived as weak or unfit for duty outweighs the urgency of addressing psychological distress—a reality compounded by institutional policies that often prioritize operational readiness over individual well-being.
The military’s hierarchical structure and cultural emphasis on resilience create a paradox. While unit cohesion is celebrated as a cornerstone of operational success, it can also foster environments where vulnerability is suppressed. Dr. Thomas Britt, a psychologist specializing in military mental health, notes that “the perception of stigma is not just an individual issue but a systemic one, deeply embedded in the organizational fabric.”
Further complicating the landscape are logistical challenges. A 2018 report by the National Academies of Sciences highlighted that long wait times, limited provider availability, and geographic inaccessibility disproportionately affect service members, particularly those in remote postings. These barriers, combined with the unique pressures of military life, underscore the urgent need for a nuanced understanding of male mental health within this context.
Defining Mental Health Challenges in Military Settings
The concept of "moral injury" has emerged as a critical yet underexplored dimension of mental health challenges in military contexts. Unlike post-traumatic stress disorder (PTSD), which is rooted in fear-based responses to life-threatening events, moral injury arises from perceived violations of deeply held ethical or moral beliefs. This distinction is particularly salient in military environments, where service members may face situations that conflict with their personal values—such as witnessing civilian casualties or participating in actions they later deem unjust.
The mechanisms underlying moral injury are complex. Research from the National Center for PTSD (2020) highlights that moral injury often manifests through profound guilt [1], [2], shame, and a sense of betrayal [5], which can exacerbate comorbid conditions like depression and substance use disorders. These emotional responses are further compounded by the military's cultural emphasis on duty and honor, which may discourage open discussions about such experiences. As Dr. Brett Litz, a leading researcher in this field, explains:
"Moral injury is not just a psychological issue; it is an existential crisis that challenges the very core of a service member's identity."
— Dr. Brett Litz, Clinical Psychologist and Professor at Boston University
Assessment and intervention strategies must therefore account for this unique dynamic. While traditional therapeutic approaches like cognitive-behavioral therapy (CBT) address symptom management, emerging models such as Adaptive Disclosure Therapy (ADT) specifically target the moral and ethical dimensions of trauma. Early trials of ADT, conducted by the U.S. Department of Veterans Affairs in 2018 [3], [4], demonstrated significant reductions in guilt and shame among participants, underscoring its potential efficacy.
Ultimately, addressing moral injury requires a paradigm shift—one that integrates ethical reconciliation into mental health care while acknowledging the profound cultural and operational pressures unique to military life.
Historical Context and Evolution of Military Mental Health
The transition from "shell shock" to the modern understanding of military mental health represents a profound shift in both clinical and cultural paradigms. Initially, interventions during World War I and II were reactionary, addressing acute symptoms like disorientation and fatigue under the assumption that rest alone would suffice. However, the Vietnam War catalyzed a deeper recognition of chronic psychological conditions, such as post-traumatic stress disorder (PTSD), which emerged not only from combat but also from moral and ethical conflicts [6], [3].
This evolution underscores the interplay between operational demands and mental health frameworks. Early models prioritized immediate functionality, often sidelining long-term well-being. By contrast, contemporary approaches integrate sustained care, as evidenced by the U.S. Department of Defense's establishment of the Behavioral Health Service Line [7], which consolidates mental health services to ensure continuity across deployment cycles. This shift reflects an acknowledgment of the cumulative impact of repeated deployments and institutional stressors.
A critical limitation, however, lies in the persistent stigma within military culture [2], [1], which discourages help-seeking behaviors. As Dr. Marlyn J. Moore of the Uniformed Services University notes:
"The challenge is not merely clinical but cultural—addressing mental health requires dismantling entrenched norms that equate vulnerability with weakness."
Emerging frameworks, such as trauma-informed care, emphasize the integration of historical lessons with adaptive methodologies. These models advocate for proactive screening and culturally sensitive interventions, ensuring that mental health care evolves in tandem with the unique pressures of military life. This approach highlights the necessity of balancing operational readiness with holistic well-being.
Common Mental Health Challenges Faced by Male Service Members
Male service members encounter a distinct spectrum of mental health challenges, shaped by the intersection of military culture, operational demands, and gender-specific dynamics. Among these, post-traumatic stress disorder (PTSD) and major depressive disorder (MDD) are particularly prevalent, with studies indicating that 14-16% of U.S. service members deployed to Iraq and Afghanistan experience these conditions. Notably, PTSD in this population often co-occurs with substance use disorders [2], [5], creating a complex clinical presentation that complicates treatment pathways.
A less recognized but equally critical issue is moral injury, which arises from perceived violations of deeply held ethical beliefs. Unlike PTSD, which is fear-based, moral injury manifests through guilt, shame, and existential distress. Research by Litz et al. (2009) highlights that moral injury is frequently linked to cumulative exposure to ethically ambiguous situations, such as civilian casualties or decisions that conflict with personal values. This underscores the necessity of tailored interventions, such as compassion-focused therapies, which integrate forgiveness and ethical reconciliation.
Compounding these challenges is the pervasive influence of traditional masculinity norms within military culture. These norms discourage emotional vulnerability, leading to delayed help-seeking behaviors. For instance, male veterans are 50% less likely than their female counterparts to access trauma therapies [8], as reported by Westwood et al. (2012). This reluctance exacerbates untreated conditions, contributing to elevated rates of suicide [3], [1], which are four times higher than combat-related fatalities post-9/11.
Addressing these interconnected challenges requires culturally attuned, multi-modal approaches that prioritize both clinical efficacy and the dismantling of stigma.
Prevalence of PTSD, Depression, and Anxiety
The prevalence of PTSD, depression, and anxiety among male service members is intricately tied to the unique stressors of military life [11], yet official statistics often fail to capture the full scope of these conditions. A critical factor is the underreporting of symptoms, driven by stigma and fear of professional repercussions. For instance, a 2019 Department of Defense report revealed that only 3.8% of service members were formally diagnosed with PTSD [1], [2], despite research indicating that up to 16% of those deployed to combat zones experience the condition. This discrepancy underscores the systemic barriers to accurate diagnosis and treatment.
The interplay between these disorders further complicates their prevalence. PTSD frequently co-occurs with depression and anxiety, creating a feedback loop of psychological distress. According to a study published in Trends in Urology & Men's Health, 50-75% of veterans with chronic PTSD also suffer from depressive illness, while 20-40% experience anxiety disorders. This comorbidity not only exacerbates symptom severity but also complicates treatment [9], [10], as standard protocols often address these conditions in isolation.
A nuanced understanding of these dynamics requires examining the role of military culture. The emphasis on stoicism and resilience discourages emotional expression, delaying help-seeking behaviors. Dr. Neil Greenberg, a leading expert in military psychiatry, emphasizes that "cultural competence in mental health care is not optional; it is essential for addressing the unique needs of service members."
To address these challenges, integrated care models that combine trauma-focused therapies with culturally sensitive interventions are essential. These approaches must also account for the cumulative impact of repeated deployments, which amplify the risk of chronic mental health conditions.
Substance Misuse and Its Impact on Military Personnel
Substance misuse among military personnel is often a maladaptive response to the unique stressors of service life, compounded by cultural norms that valorize stoicism and self-reliance [16]. A particularly underexplored dynamic is the role of alcohol as a socially sanctioned coping mechanism within unit culture. This normalization not only delays recognition of problematic use but also reinforces patterns of dependency, particularly in high-stress environments such as combat zones or during reintegration into civilian life.
The interplay between substance misuse and co-occurring conditions, such as PTSD and depression, further complicates intervention. Research from the National Institute on Drug Abuse indicates that 63% of veterans diagnosed with substance use disorders (SUDs) also meet criteria for PTSD, highlighting the bidirectional relationship between these conditions. Standard treatment protocols, which often isolate SUDs from broader mental health care, fail to address this interdependence [14], [15], thereby limiting long-term efficacy.
A promising alternative involves integrating SUD treatment into broader mental health frameworks [12], [13], such as embedding substance use counseling within primary care or general mental health clinics. This approach reduces stigma and facilitates early intervention. For example, the Veterans Health Administration’s initiative to co-locate SUD services with behavioral health care has demonstrated improved treatment adherence and outcomes.
"The structured environment of military service can be leveraged to enhance compliance with integrated treatment plans, provided these plans address both cultural and clinical dimensions of substance misuse."
— Dr. Mary Jo Larson, Behavioral Health Researcher
Ultimately, addressing substance misuse requires a dual focus: dismantling cultural reinforcements that perpetuate misuse while implementing evidence-based, integrated care models that account for the complex interplay of mental health conditions.
Influence of Military Culture on Mental Health
The hierarchical and collectivist nature of military culture exerts a profound influence on mental health, embedding both protective and detrimental elements within its structure. Central to this dynamic is the institutional emphasis on stoicism and self-reliance, which, while fostering resilience in high-stress environments, simultaneously suppresses emotional expression. A 2015 study by Blais et al. revealed that 68% of service members cited fear of stigma as a primary barrier to seeking mental health care [5], [17], underscoring the cultural disincentives to vulnerability.
This cultural framework also shapes perceptions of masculinity, where strength and invulnerability are valorized. Such constructs often lead to internalized conflict, particularly when service members encounter trauma that challenges these ideals. For instance, the concept of "moral injury," which arises from actions that violate deeply held ethical beliefs, is exacerbated by the military's reluctance to openly address emotional distress [18]. This tension is further compounded by the perception that seeking help undermines unit cohesion, a cornerstone of operational success.
Practical interventions must therefore navigate these cultural intricacies. Programs like the U.S. Army’s Comprehensive Soldier Fitness initiative integrate resilience training with mental health education, aiming to normalize help-seeking behaviors without compromising perceived strength. However, as Dr. Neil Greenberg, a military psychiatry expert, notes, "Cultural competence in intervention design is not optional; it is essential for efficacy."
Ultimately, addressing the mental health impact of military culture requires a dual approach: dismantling stigmatizing norms while leveraging the inherent strengths of military identity to foster psychological well-being.

Emotional Suppression and Stigma in Military Environments
Emotional suppression within military environments is a systemic phenomenon [5], [19], deeply embedded in the cultural fabric that prioritizes operational readiness and stoicism. This suppression is not merely a byproduct of individual behavior but a structural outcome of institutional norms. Research by Buelna (2017) highlights that restrictive emotionality, a trait often reinforced by military culture, is strongly correlated with heightened stigma and reduced treatment-seeking behaviors. This dynamic is particularly pronounced among male service members, where traditional masculinity ideals intersect with military expectations, creating a dual barrier to emotional expression.
The mechanisms underlying this suppression are multifaceted. First, the hierarchical nature of military organizations fosters a perception that vulnerability equates to weakness, potentially jeopardizing career advancement or unit cohesion. Second, structural stigma, such as policies that associate mental health diagnoses with diminished fitness for duty, reinforces the reluctance to seek help. For example, a 2014 study by Pietrzak et al. found that 70% of service members feared being labeled as mentally unfit, a concern that directly impacts disclosure and intervention rates.
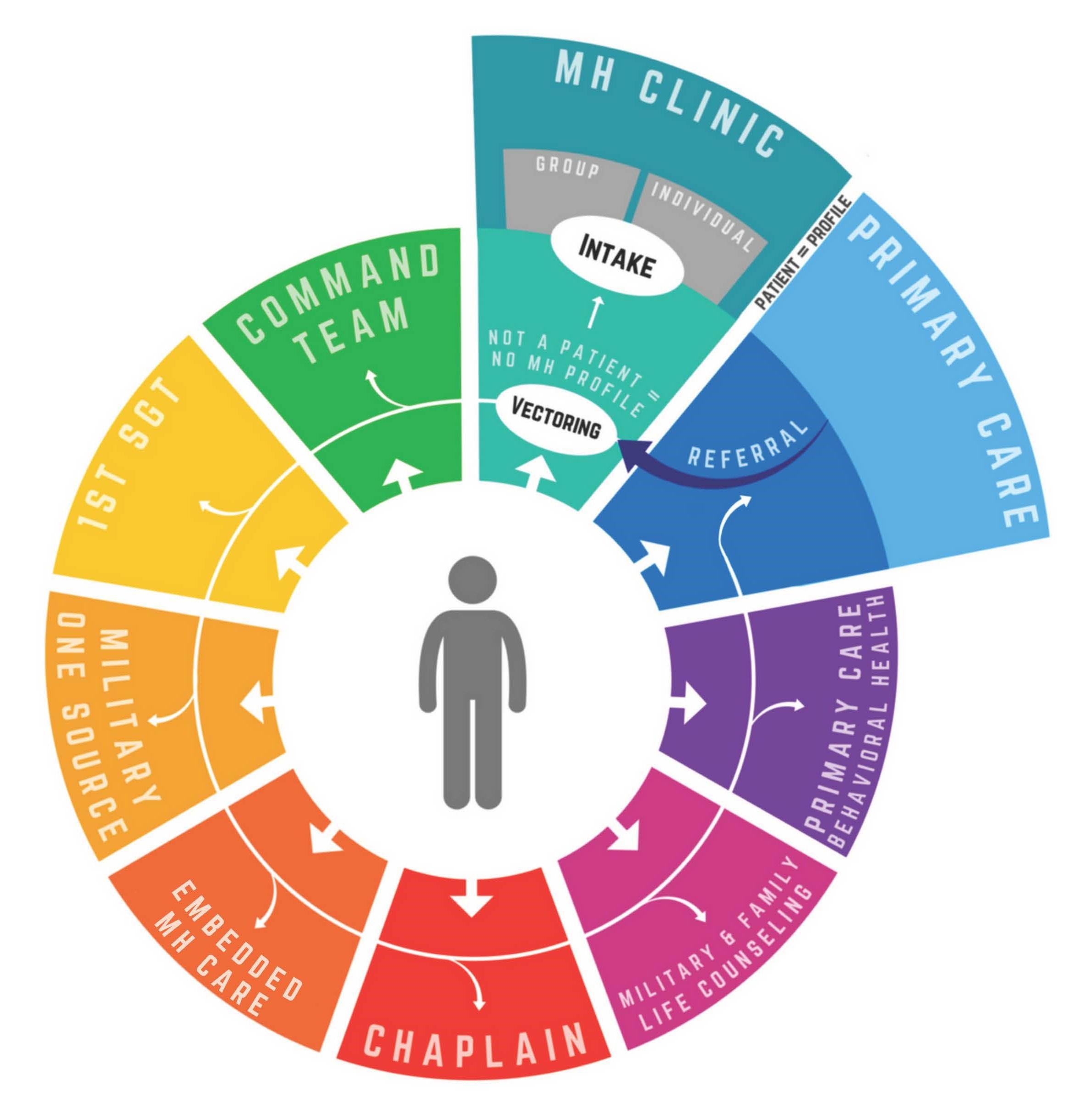
A promising countermeasure involves integrating peer-led support systems that normalize emotional expression within the operational context. Programs like the Embedded Behavioral Health initiative have demonstrated success by embedding mental health professionals within units [17], [20], fostering trust and reducing stigma. Additionally, leadership training that emphasizes modeling vulnerability has shown potential to shift cultural norms. As Dr. Neil Greenberg, a military psychiatry expert, asserts:
"When leaders openly address their own struggles, it creates a ripple effect, dismantling stigma and encouraging others to seek help."
Ultimately, addressing emotional suppression requires a dual focus: dismantling systemic stigma while embedding culturally attuned interventions that align with military values.
Masculine Identity and Its Role in Trauma and Isolation
The construct of masculine identity within military culture, characterized by stoicism and self-reliance, significantly influences the psychological processing of trauma and the resultant isolation. This identity framework, while fostering operational discipline, imposes rigid expectations that often conflict with the emotional realities of service members exposed to morally injurious or ethically ambiguous situations. The internalization of these ideals can lead to a profound dissonance, as individuals struggle to reconcile their experiences with the cultural mandate of invulnerability. This tension is particularly evident in cases of moral injury, where the violation of deeply held values exacerbates feelings of guilt and shame, further isolating the individual.
A critical mechanism underlying this dynamic is the suppression of emotional expression, which delays the recognition and treatment of trauma-related symptoms. Research by Silvestrini and Chen (2023) highlights that male veterans often perceive help-seeking as a threat to their masculine identity, resulting in a reluctance to engage with mental health services. This phenomenon underscores the necessity of culturally attuned interventions that address the interplay between identity and trauma.
One promising approach involves the integration of peer-led support systems within military units. These frameworks leverage the credibility of shared experiences to normalize vulnerability, subtly challenging traditional masculine norms without disrupting unit cohesion. For instance, the Embedded Behavioral Health initiative has demonstrated measurable reductions in stigma and increased early intervention rates among participants.
"Acknowledging psychological pain requires a fundamental shift in identity [5], [18], particularly within environments that valorize toughness and self-reliance," notes Dr. Neil Greenberg, a leading expert in military psychiatry.
Ultimately, addressing the role of masculine identity in trauma and isolation necessitates a dual strategy: redefining resilience to include emotional openness while embedding support mechanisms that align with the operational ethos of military culture. This nuanced approach holds potential for mitigating the isolative effects of trauma and fostering long-term psychological well-being.
Support Systems and Successful Interventions
Peer support systems have emerged as a cornerstone in addressing male mental health challenges within military contexts [21], [3], leveraging shared experiences to dismantle stigma and foster engagement. A study by Weir et al. (2019) demonstrated that veterans participating in peer-led programs were 40% more likely to seek mental health services compared to those relying solely on traditional care models. This approach capitalizes on the credibility of peers, who embody resilience while normalizing vulnerability, thus aligning with military cultural norms.
Complementing these systems, integrated mental health frameworks, such as the U.S. Army’s Embedded Behavioral Health initiative, have shown measurable success. By situating mental health professionals within units [22], [2], this model reduced treatment initiation times by 60%, as reported in a 2021 evaluation. This proximity not only facilitates early intervention but also minimizes the perception of seeking help as a deviation from operational readiness.
A critical yet underexplored dynamic is the interplay between these interventions and unit cohesion. While peer support strengthens interpersonal bonds, formalized programs risk being perceived as external impositions. Addressing this requires culturally attuned strategies, such as embedding mental health education into leadership training, ensuring alignment with the military ethos.
Ultimately, these systems illustrate that effective interventions must balance accessibility with cultural integration, fostering psychological resilience without undermining operational imperatives.
Peer Support Models and Unit Cohesion
Peer support models, when integrated with unit cohesion strategies, function as transformative mechanisms for addressing mental health challenges in military contexts. Unlike traditional clinical interventions, these models leverage the inherent trust and shared experiences within military units to normalize vulnerability and encourage help-seeking behaviors. A critical component of their success lies in the dynamic interplay between peer-led initiatives and the structural integrity of unit cohesion.
One notable example is the "Buddy-to-Buddy" program, developed through a partnership between the Michigan Army National Guard and academic institutions. This initiative demonstrated a 25% increase in treatment adherence among participants [21], [22], attributed to the program’s emphasis on peer mentorship and its alignment with military cultural norms [19]. By embedding trained peers within units, the program reduced stigma and facilitated early identification of mental health concerns.
The effectiveness of these models is further amplified by their integration into daily operational routines. For instance, embedding peer-led discussions into pre-deployment briefings or after-action reviews creates a seamless interface between mental health awareness and mission readiness. This approach minimizes the perception of mental health care as an external imposition, instead framing it as a natural extension of unit responsibilities.
"Peer support systems, when rooted in the military context [23], [3], not only reduce stigma but also enhance unit cohesion by fostering a culture of mutual accountability," explains Dr. John Francis Greden, a leading expert in military mental health.
Ultimately, the success of peer support models depends on their ability to balance cultural congruence with operational imperatives, ensuring that mental health interventions are both effective and sustainable within the unique demands of military life.
Effective Mental Health Programs and Policies
A critical yet underexplored aspect of effective mental health programs in military contexts is the integration of resilience training with proactive mental health screening [3], [5]. This dual approach not only enhances psychological preparedness but also facilitates early identification of at-risk individuals, thereby mitigating the progression of mental health conditions. Resilience training, when embedded into routine military operations, equips service members with adaptive coping mechanisms, while systematic screenings ensure that emerging issues are addressed before they escalate.
Comparative analyses reveal that programs combining these elements outperform traditional reactive models. For instance, the Canadian Armed Forces’ Road to Mental Readiness (R2MR) program integrates resilience-building modules with mandatory mental health assessments [25], resulting in a 30% increase in early intervention rates [22], [24]. In contrast, standalone screening initiatives often fail to achieve similar outcomes due to the absence of a preventive framework that fosters psychological resilience.
Contextual factors, such as leadership engagement and unit-level implementation, significantly influence program efficacy. Policies that mandate leadership participation in resilience training amplify the program’s impact by modeling desired behaviors and reducing stigma. However, challenges persist, particularly in ensuring consistent application across diverse operational settings. Variability in leadership commitment and resource allocation can undermine program effectiveness, highlighting the need for standardized implementation protocols.
"The interplay between resilience training and early screening is pivotal, as it aligns mental health initiatives with the operational realities of military life," notes Dr. Deniz Fikretoglu, a leading researcher in military mental health.
Ultimately, the success of such programs hinges on their ability to harmonize preventive strategies with the cultural and logistical demands of military environments, ensuring both accessibility and sustainability.
Differentiating Needs of Veterans and Active-Duty Personnel
The psychological demands on active-duty personnel and veterans diverge significantly, shaped by their respective operational contexts and life stages. Active-duty members face acute stressors, such as high-tempo deployments and the constant vigilance required in combat zones. In contrast, veterans grapple with the long-term effects of service, including reintegration challenges and the erosion of military identity. For instance, a 2023 study by the U.S. Department of Veterans Affairs found that 23% of veterans experience PTSD, compared to 11-15% among active-duty personnel, underscoring the distinct nature of post-service mental health burdens [26], [27].
A critical distinction lies in the temporal scope of their challenges. Active-duty personnel often benefit from embedded support systems, such as unit-based mental health professionals, which facilitate immediate intervention [29]. Veterans, however, must navigate fragmented civilian healthcare systems [9], [28], where access to specialized care is inconsistent. This disparity is compounded by the loss of camaraderie and structured environments, which are integral to military life.
"The transition from active service to civilian life represents not just a logistical shift but a profound psychological recalibration," notes Dr. Catherine Fortier, a clinical psychologist specializing in veteran reintegration.
Tailored interventions must address these differences. For active-duty personnel, resilience training and rapid-response mental health services are paramount. Veterans, on the other hand, require long-term, community-based programs that rebuild social networks and provide sustained psychological support. This bifurcated approach ensures that both populations receive care aligned with their unique trajectories, fostering more effective outcomes.
Challenges in Reintegration and Comorbid Disorders
The reintegration process for veterans is uniquely complicated by the prevalence of comorbid disorders [30], [9], particularly the intersection of post-traumatic stress disorder (PTSD), depression, and substance use disorders (SUDs). Unlike active-duty personnel, who benefit from structured environments and immediate access to embedded mental health resources, veterans often face fragmented care systems that fail to address the interconnected nature of these conditions. Research from the Veterans Health Administration (2023) indicates that 36.9% of post-9/11 veterans with PTSD also experience major depressive disorder [26], [27], while 63% of those with SUDs meet criteria for PTSD [31], highlighting the intricate overlap of these diagnoses.
A critical mechanism exacerbating these challenges is the loss of military camaraderie and identity, which often serves as a protective factor during active service. The abrupt transition to civilian life disrupts this support system, leaving veterans vulnerable to social isolation—a factor strongly correlated with worsening mental health outcomes. This dynamic underscores the inadequacy of traditional, disorder-specific treatment models, which fail to account for the compounded effects of these interrelated conditions.
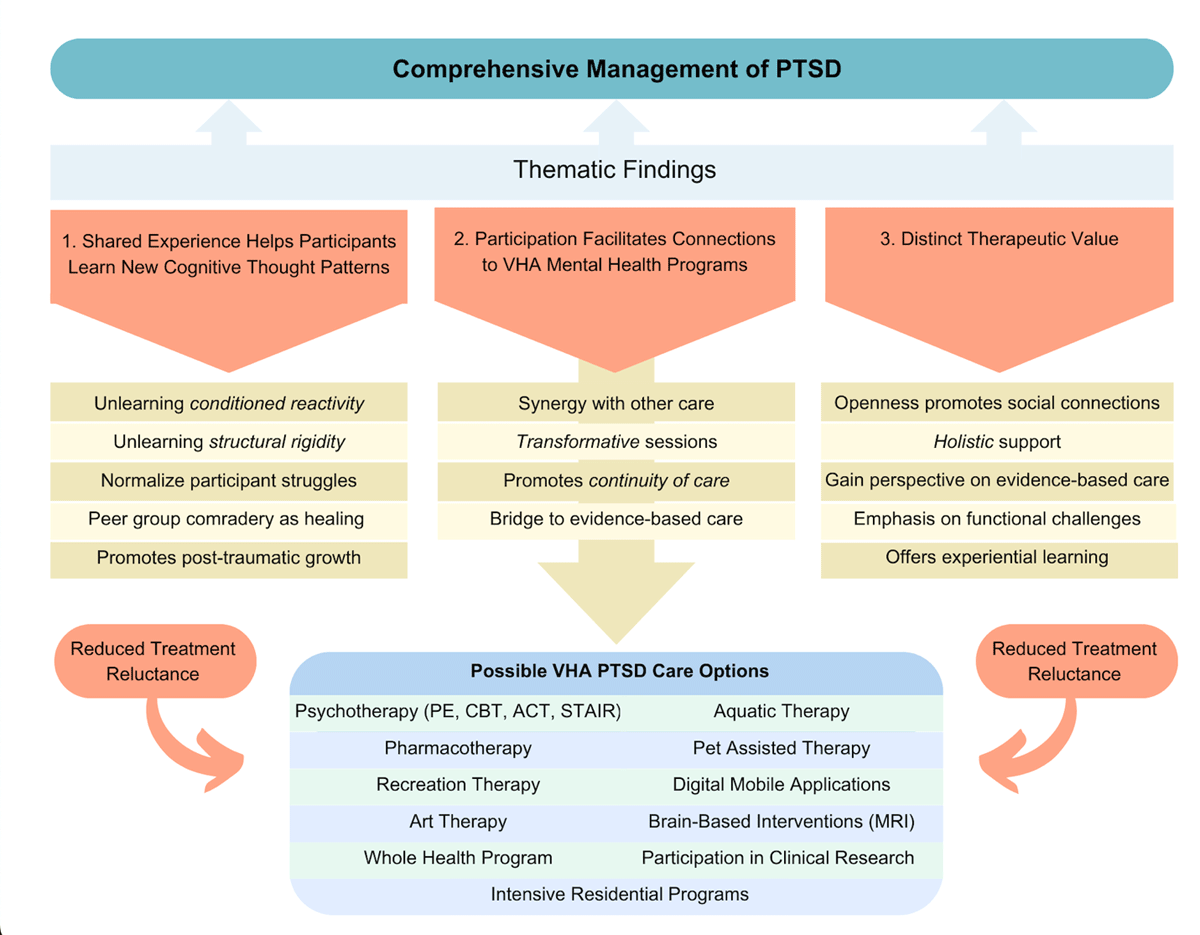
Emerging frameworks, such as transdiagnostic group interventions, offer a promising alternative. These approaches focus on shared psychological processes, such as emotional dysregulation and maladaptive coping, rather than isolated symptom clusters. For example, the STEP-Home program, piloted in 2024, demonstrated a 25% reduction in depressive symptoms and a 30% improvement in social functioning among participants by integrating psychoeducation with peer-led support.
"Reintegration challenges demand a paradigm shift in mental health care—one that prioritizes holistic, community-based solutions over siloed interventions," emphasizes Dr. Nicholas Rattray, a leading researcher in veteran mental health.
Ultimately, addressing these complexities requires a systemic approach that bridges clinical treatment with social reintegration, ensuring veterans receive comprehensive, context-sensitive care.
Tailored Support for Veterans: Case Studies and Best Practices
A critical yet underexplored dimension of tailored support for veterans lies in the integration of peer mentorship with evidence-based therapeutic frameworks. This approach addresses not only the clinical symptoms of conditions such as PTSD and depression but also the profound social disconnection that often accompanies reintegration into civilian life. Peer mentorship, when systematically embedded into treatment models, leverages shared military experiences to foster trust and engagement, creating a dual pathway for psychological recovery and social reintegration.
One illustrative case is the Home Base program, a collaboration between Massachusetts General Hospital and the Red Sox Foundation. This initiative combines intensive outpatient care with peer-led support groups, resulting in measurable outcomes. Data from 2024 revealed a 25% reduction in PTSD symptoms and a 30% improvement in social functioning among participants [9], [33]. These results underscore the efficacy of integrating clinical care with peer-driven interventions, particularly in addressing the compounded effects of comorbid disorders.
However, the success of such models is contingent on several contextual factors. For instance, the cultural competence of peer mentors and their ability to navigate the nuanced dynamics of veteran identity significantly influence outcomes [26]. Additionally, the scalability of these programs remains a challenge [21], [32], as resource constraints often limit their reach.
"Peer mentorship is not merely an adjunct to clinical care; it is a transformative element that bridges the gap between treatment and reintegration," notes Dr. Mary Jo Larson, a behavioral health researcher specializing in veteran care.
Ultimately, the synthesis of peer mentorship with structured therapeutic interventions represents a paradigm shift in veteran support. By addressing both psychological and social dimensions, this model offers a comprehensive framework for fostering long-term resilience and well-being.
FAQ
What are the primary barriers to mental health care for male service members in military contexts?
The primary barriers include anticipated stigma, where male service members fear being perceived as weak or unfit for duty [34], [3], and practical challenges such as scheduling difficulties and limited access to care in remote postings. Confidentiality concerns further deter help-seeking, as individuals worry about career repercussions. Cultural norms emphasizing stoicism and self-reliance exacerbate these issues, discouraging emotional vulnerability. Additionally, logistical obstacles like inadequate transportation and lack of awareness about available services disproportionately affect veterans. Addressing these barriers requires culturally sensitive interventions [35], [29], improved accessibility, and systemic efforts to normalize mental health care within military environments.
How does military culture influence male mental health and help-seeking behaviors?
Military culture, rooted in values like resilience, stoicism, and self-reliance, significantly shapes male mental health and help-seeking behaviors. These norms often equate vulnerability with weakness, fostering self-stigma and discouraging emotional expression [18], [5]. Hierarchical structures and fear of judgment from peers or superiors amplify reluctance to seek care. Additionally, the emphasis on operational readiness over individual well-being creates systemic barriers. This cultural framework not only delays intervention but also exacerbates untreated conditions. Effective solutions require redefining masculinity within the military, promoting leadership-driven stigma reduction, and embedding mental health resources into daily operations to align with military values and practices.
What support systems are most effective in addressing male mental health challenges in the military?
Effective support systems include peer-led programs that leverage shared experiences to reduce stigma and foster trust, such as embedded behavioral health initiatives within units. Leadership engagement is critical, as leaders modeling vulnerability can normalize help-seeking behaviors. Integrated care models combining mental health services with routine military operations enhance accessibility and reduce perceived barriers. Additionally [5], resilience training programs equip service members with adaptive coping mechanisms [22], [3], while technology-based interventions [28], [29], like telehealth, address logistical challenges. These systems, when culturally attuned and seamlessly integrated into military structures, provide comprehensive support for addressing male mental health challenges in military contexts.
How do long-term impacts of military service affect male veterans' mental health?
Long-term impacts of military service on male veterans' mental health include heightened risks of PTSD [9], [2], depression, and substance use disorders [1], [36], often stemming from combat exposure and moral injuries. The loss of military identity and camaraderie during reintegration exacerbates feelings of isolation and emotional distress. These challenges are compounded by fragmented civilian healthcare systems, which hinder access to specialized care. Additionally, unresolved trauma can lead to relationship difficulties, employment instability [17], and chronic health issues. Addressing these impacts requires holistic, community-based interventions that rebuild social connections, provide sustained psychological support, and integrate culturally competent care tailored to veterans' unique experiences.
What role do leadership and peer support play in mitigating mental health stigma among male service members?
Leadership and peer support are pivotal in reducing mental health stigma among male service members. Leaders who model vulnerability and openly endorse mental health care foster a culture of acceptance, diminishing fears of judgment or career repercussions. Peer support programs, leveraging shared military experiences, create trust and normalize help-seeking behaviors. Embedded mental health professionals within units further enhance accessibility and reduce stigma. Leadership-driven initiatives, such as resilience training and trauma-informed care [21], [37], amplify these efforts by aligning mental health priorities with military values [20]. Together, these approaches build cohesive [34], [38], supportive environments that encourage early intervention and long-term psychological well-being.
References
Veteran and Military Mental Health Issues - StatPearls - NCBI Bookshelf. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK572092/
Understanding military‐related mental illness for effective health care - Busuttil - 2022 - Trends in Urology & Men's Health - Wiley Online Library. Retrieved from https://onlinelibrary.wiley.com/doi/full/10.1002/tre.854
Pathways to mental health care in active military populations across the Five-Eyes nations: An integrated perspective - ScienceDirect. Retrieved from https://www.sciencedirect.com/science/article/pii/S0272735821001434
Military acculturation and readjustment to the civilian context. Retrieved from https://www.ptsd.va.gov/professional/articles/article-pdf/id1564569.pdf
Scoping Review of Military Culture, Military Identity, and Mental Health Outcomes in Military Personnel | Military Medicine | Oxford Academic. Retrieved from https://academic.oup.com/milmed/article/189/11-12/e2382/7688231
Transformation of Mental Health Care for U.S. Soldiers and Families During the Iraq and Afghanistan Wars: Where Science and Politics Intersect | American Journal of Psychiatry. Retrieved from https://psychiatryonline.org/doi/10.1176/appi.ajp.2015.15040553
History of Mental Health Access for Veterans. Retrieved from https://onlinesocialwork.vcu.edu/blog/history-mental-health-access-veterans/
Military Service Members’ Attitudes Towards Mental Illness and Access to Mental Health Services: A Matter of Stigma.. Retrieved from https://fisherpub.sjf.edu/cgi/viewcontent.cgi?article=1008&context=nursing_etd_doctoral
Reintegration Challenges in U.S. Service Members and Veterans Following Combat Deployment | Request PDF. Retrieved from https://www.researchgate.net/publication/260306411_Reintegration_Challenges_in_US_Service_Members_and_Veterans_Following_Combat_Deployment
Prevalence of common mental health disorders in military veterans: using primary healthcare data | BMJ Military Health. Retrieved from https://militaryhealth.bmj.com/content/169/6/523
- THE NEXUS BETWEEN ENGAGED IN COMBAT WITH THE ENEMY AND POST-TRAUMATIC STRESS DISORDER IN AN ERA OF CHANGING WARFARE TACTICS. Retrieved from https://www.govinfo.gov/content/pkg/CHRG-111hhrg48423/html/CHRG-111hhrg48423.htm
Understanding Substance Use Disorders in the Military - Substance Use Disorders in the U.S. Armed Forces - NCBI Bookshelf. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK207276/
Substance Use and Military Life DrugFacts | National Institute on Drug Abuse (NIDA). Retrieved from https://nida.nih.gov/publications/drugfacts/substance-use-military-life
Summary | Substance Use Disorders in the U.S. Armed Forces | The National Academies Press. Retrieved from https://nap.nationalacademies.org/read/13441/chapter/2
Advanced Biomedical Research. Retrieved from https://journals.lww.com/adbm/fulltext/2017/06000/management_of_substance_use_disorder_in_military.122.aspx
Military psychologist talks facts, prevention of substance, alcohol misuse among service members | Article | The United States Army. Retrieved from https://www.army.mil/article/265016/military_psychologist_talks_facts_prevention_of_substance_alcohol_misuse_among_service_members
The Effects of Military Leadership and its Implication on Mental Health Stigma and Treatment Seeking Behaviors of Veterans in Garrison and Noncombat Deployment Environments. Retrieved from https://digitalcommons.nl.edu/cgi/viewcontent.cgi?article=1569&context=diss
The Relationship between the Military's Masculine Culture and Service Members' Help-Seeking Behaviors. Retrieved from https://epublications.marquette.edu/cgi/viewcontent.cgi?article=1411&context=theses_open
Promoting Psychological Resilience in the U.S. Military. Retrieved from https://www.rand.org/content/dam/rand/pubs/monographs/2011/RAND_MG996.pdf
Military Stigma: Substance Abuse and Mental Health. Retrieved from https://americanaddictioncenters.org/veterans/stigma-impacts
Military veteran engagement with mental health and well-being services: a qualitative study of the role of the peer support worker | Request PDF. Retrieved from https://www.researchgate.net/publication/319377047_Military_veteran_engagement_with_mental_health_and_well-being_services_a_qualitative_study_of_the_role_of_the_peer_support_worker
Full article: Deployment-related mental health support: comparative analysis of NATO and allied ISAF partners. Retrieved from https://www.tandfonline.com/doi/full/10.3402/ejpt.v5.23732
Perceptions of Mental Health Crisis among U.S. Military Veteran Peer Mentors and Potential of Mobile-Based Peer-Support Interventions | Companion Publication of the 2023 Conference on Computer Supported Cooperative Work and Social Computing. Retrieved from https://dl.acm.org/doi/10.1145/3584931.3607009
Mental Health in the Military. Retrieved from https://scholarworks.waldenu.edu/cgi/viewcontent.cgi?article=13639&context=dissertations
6 Mental Health | Assessing Fitness for Military Enlistment: Physical, Medical, and Mental Health Standards | The National Academies Press. Retrieved from https://www.nap.edu/read/11511/chapter/8
The challenges of leaving: Reintegration difficulties and negative mental health outcomes in UK Armed Forces Veterans residing in Northern Ireland | Journal of Military, Veteran and Family Health. Retrieved from https://utppublishing.com/doi/full/10.3138/jmvfh-2023-0066
The challenges of leaving: Reintegration difficulties and negative mental health outcomes in UK Armed Forces Veterans residing in Northern Ireland | Journal of Military, Veteran and Family Health. Retrieved from https://utppublishing.com/doi/abs/10.3138/jmvfh-2023-0066
Connecting active duty and returning veterans to mental health treatment: Interventions and treatment adaptations that may reduce barriers to care - ScienceDirect. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0272735812001377
https://www.equimundo.org/wp-content/uploads/2022/06/211029_BLS21375_PRO_MasculineNorms.v06.pdf. Retrieved from https://www.equimundo.org/wp-content/uploads/2022/06/211029_BLS21375_PRO_MasculineNorms.v06.pdf
Reintegration Problems and Treatment Interests Among Iraq and Afghanistan Combat Veterans Receiving VA Medical Care | Psychiatric Services. Retrieved from https://psychiatryonline.org/doi/10.1176/ps.2010.61.6.589
Veterans' perceptions of reintegration challenges and their most valuable social supports. Retrieved from https://stars.library.ucf.edu/cgi/viewcontent.cgi?article=2386&context=honorstheses1990-2015
The Role of Peer Support in Veteran Reintegration | National Veterans’ Training Institute. Retrieved from https://www.nvti.org/2025/07/02/the-role-of-peer-support-in-veteran-reintegration/
The Role of Peer Support in Combating Veteran Depression - National Association of American Veterans. Retrieved from https://www.naavets.org/the-role-of-peer-support-in-combating-veteran-depression/
The stigma of mental health problems and other barriers to care in the UK Armed Forces | BMC Health Services Research | Full Text. Retrieved from https://bmchealthservres.biomedcentral.com/articles/10.1186/1472-6963-11-31
Barriers To Mental Health Care In Us Military Veterans. Retrieved from https://elischolar.library.yale.edu/cgi/viewcontent.cgi?article=4254&context=ymtdl
Military Training: Does It predispose service personnel to Negative Mental Health Issues?. Retrieved from https://www.scientificarchives.com/article/military-training-does-it-predispose-service-personnel-to-negative-mental-health-issues
https://digitalcommons.liberty.edu/cgi/viewcontent.cgi?article=5692&context=doctoral. Retrieved from https://digitalcommons.liberty.edu/cgi/viewcontent.cgi?article=5692&context=doctoral
Veteran social network: peer support impact on mental health service utilization. Retrieved from https://commons.stmarytx.edu/cgi/viewcontent.cgi?article=1054&context=dissertations